Great and Desperate Cures: The Rise and Decline of Psychosurgery and Other Radical Treatments for Mental Illness
I. SURGERY FOR THE SOUL
Surgery for the soul required a sharp, eight-inch-long instrument—one time, an ice pick from the Uline Ice Company was used—and not much else. It did not require anesthesia or gloves, and the sharp instrument (either a leucotome or the sturdier orbitoclast) was not necessarily sterilized. It took less than ten minutes.
The first step was to shock the patient until they lost consciousness. This eliminated the need for anesthesia, since there would be at least a few minutes until the patient regained consciousness, and also made the procedure more flexible; it did not require a surgeon, and did not even have to be performed in a hospital.
The second step was to insert the sharp, eight-inch-long instrument into the brain. In most versions of the procedure, surgeons drilled holes into the skull and inserted the leucotome through those holes. Surgeons preferred an approach that allowed them to see where in the brain they were cutting. But the abbreviated procedure used a shortcut.
Just above and behind the eye is a thin plate of bone that forms the roof of the eye socket. With enough force, the leucotome can be driven through that bone and into the frontal lobes of the brain. The cracking sound produced when the instrument fractures the orbital roof has caused at least one experienced clinician to faint.
Once the instrument was inside, completing the surgery was simply a matter of rotating the tool left and right. The goal was to cut a large number of nerve fibers. Some thought that the procedure might work by severing fibers which maintained certain fixed distorted thought patterns; by destroying them, patients might be freed from the grip of their mental illness. But there wasn’t agreement among practitioners regarding why the procedure might work.
This is the transorbital lobotomy. Around 50,000 people received lobotomies in the United States in the 1940s and early 1950s; approximately 10,000 used the transorbital method I just described, with the others using approaches surgeons would be more likely to approve of (e.g., using anesthesia, gloves, being able to see where you’re cutting…).
It was billed as a cure for all sorts of mental illnesses, including schizophrenia, depression, and anxiety. And while some called it a method of last resort—a procedure which should only be used after every other conceivable method had failed—it was often used on people who did not have serious mental problems, and who had not tried less serious treatments.
In a particularly egregious case, a twelve year-old boy received a lobotomy, essentially because his stepmother did not like him. Here he is before, during, and after his surgery:



He has black eyes in the ‘after’ picture because the metal leucotome had been shoved into his eye sockets, and through the bony orbits, in order to reach his brain. This boy survived, had an extremely difficult life, and decades later wrote a memoir called My Lobotomy. Here’s an excerpt from the notes of the doctor that performed the procedure:
He came around quickly after the first shock and I eventually gave him 4, after which he was quite slow in recovering, with some cyanosis and rattling in the chest. I think it was one more than necessary. I introduced the orbitoclasts under the eyelids 3 cm from the midline, aimed them parallel with the nose and drove them to a depth of 5 cm. I pulled the handles laterally, returned them half way and drove them 2 cm deeper. Here I touched the handles over the nose, separated them 45 degrees and elevated them 50 degrees, bringing them parallel for photography before removal. There was an escape of a small amount of blood-stained fluid from each side. Howard did not get much swelling or discoloration from the eyelids; however, he did have a considerable amount of vomiting during the night and I prescribed dramamine 50 mg for its control. When I saw him this morning he recognized me but thought he was on Orange Street and that the day was Monday instead of Saturday. He did not know that anything particular had happened to him. He'd been incontinent once during the night. He resisted efforts to get his eyes open and complained about the needles that were being given him. His temperature, pulse and respiration were quite normal, and the neurologic picture was OK.
It is surprising that the results of the surgery were not universally negative. Some people really did claim to have been helped by the procedure. Some were able to return to society and work real jobs. But most were not. If the surgery did nothing, you were lucky, since it often resulted in serious incapacitation. Patients were no longer able to take care of themselves. Their personalities were destroyed. Some vibrant spark which formed a core part of their humanity was lost in the process of surgery for the soul.
The lobotomy may be the most harmful, infamous, evil ‘treatment’ in the history of modern medicine. Why was it allowed to happen? Why would anyone ever think it was a good idea?
II. SYMPATHY FOR THE DEVIL
The mission of Great and Desperate Cures (1986), a book by the psychologist and neuroscientist Elliot Valenstein, is to provide a thorough answer to these questions. It’s a weird book: it’s not a dumbed-down popular science book, and while Valenstein clearly made some effort to make the content palatable to a wider audience, entertainment is not his main or even secondary objective. In some places it feels like Valenstein doesn’t really care if anyone reads the book. He just wants to get to the bottom of this. Why was this allowed to happen?
Also, the cover of the book is cool. The illustration recalls Saturn Devouring His Son by Goya.
The reasons Valenstein comes up with are not extremely surprising. There are six:
(i) desperate patients and families, who were open to anything that might help;
(ii) the pull of “fame and name” for ambitious physicians;
(iii) the uncritical acceptance by clinicians of lobotomy-related claims;
(iv) the uncritical acceptance by the media of lobotomy-related claims and the subsequent overenthusiastic promotion of lobotomy;
(v) territorial disputes between competing subfields with different views on how mental illness ought to be conceived; and
(vi) coldblooded economics, especially regarding the cost of patient care in overcrowded and underfunded state hospitals for the mentally ill.
But the details are compelling. They are insane. I have never read anything quite like this.
The thesis of Great and Desperate Cures is that there is something banal about the lobotomy, and efforts in psychosurgery—physically intervening on the brain in order to treat mental illness—more generally. Brains were mutilated not through the schemes of rogue physicians with kooky ideas, but by decorated, well-informed, and talented physicians who (at least in some cases) based their work on then-current theories of the brain. To be sure, the story is full of colorful and shady characters whose desire for “fame and name” led them to play fast and loose with the lives of their patients. It is true that their efforts at promoting themselves, and surgeries like the lobotomy that they were associated with, played a role in the spread and normalization of psychosurgery.
But one gets the sense from Valenstein that in an alternate universe where things happened differently, perhaps because one of the key players never existed or became a painter instead of a physician, the situation would not have been that different. Someone would have done it. The demand was too great and the safeguards were too few.
The most effective illustration of this, I think, is the reason lobotomies stopped. Despite the horrors of the procedure, and despite the mixed-to-negative outcomes—in tens of thousands of cases—they only really stopped because they were replaced. In 1954, the antipsychotic drug chlorpromazine was approved by the Food and Drug Administration and became widely available for physicians to prescribe. Although they could not address every problem proponents of psychosurgery claimed to be able to address, the overlap between use cases was still fairly high. Lobotomies stopped not because there was some huge reckoning within the medical community, but because they were effectively outcompeted by a simpler, cheaper, less permanent treatment option.
Great and Desperate Cures was released in 1986. Forty years later, in 2026, how relevant are the factors Valenstein identified? Could anything like a lobotomy happen today? Let’s go through them, one at a time, to see.
I also just want an excuse to talk about some of the history discussed in this book. It is insane. I have never read anything quite like this. I have to say that a second time so you know I really mean it.
III. DESPERATION
Anyone attempting to sympathize with the perpetrators of the lobotomy must place it in its proper historical context. The leucotomy—the direct precursor of the lobotomy whose difference in name is more branding than anything else—was first performed on patients in 1935, nearly a hundred years ago. As mysterious as the brain is now, it was significantly more mysterious in the 1930s. This was a time well before any theories of neural computation, before our understanding of the structure of DNA and molecular biology, and still two decades before the first psychoactive drugs. Freudian psychoanalysis was still a dominant force in shaping the way clinicians thought about mental illness, but it would be more accurate to say that many things affected people’s views; there was no single overwhelmingly successful paradigm.
Mental illness, both in the early twentieth century and now, is a major problem. Millions of people are violent, self-destructive, delusional, incoherent, unable to take care of themselves, or some combination of those things. In the 1930s, when the lobotomy was conceived and first performed, the United States was still dotted with insane asylums. These were government solutions to a social problem: they offered a ‘home’ for mentally ill people with no other place to go. Famously, the conditions in many of these places were deplorable. They were dirty, loud, cramped, understaffed, and sick and vulnerable patients were not always treated with kindness and gentleness.
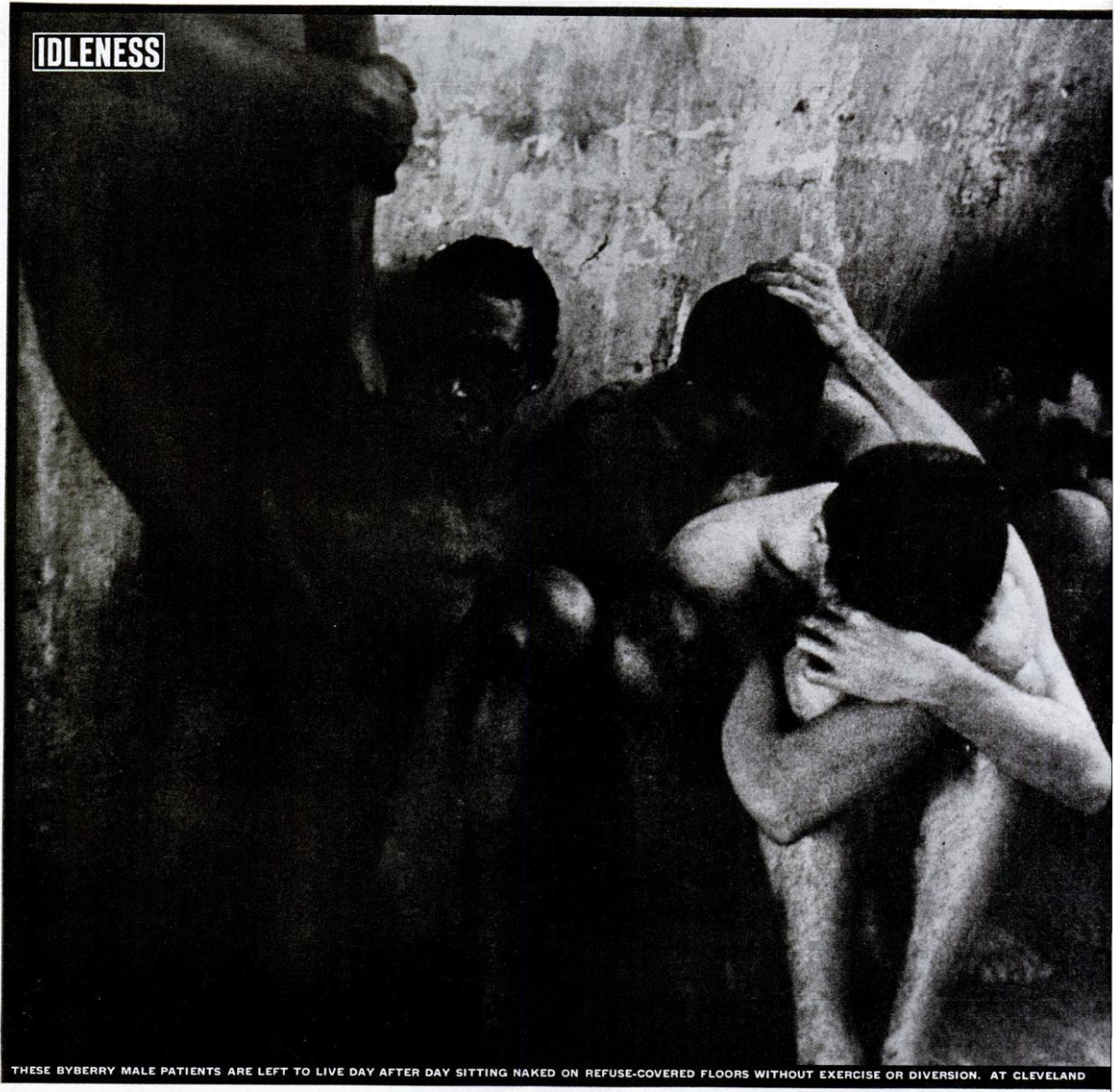
Image from a May 6, 1946 expose in Life magazine. (source)
Valenstein explains: (ch. 9, pp. 175-177)
The American Psychiatric Association estimated overcrowding in mental hospitals even in 1948 to be in excess of 50 percent. More than 230,000 hospital beds for the mentally ill were judged to be substandard, and many more people needed hospitalization. William Menninger reported that there were 700,000 beds for mental patients in the United States; but that hospitalization of everyone needing intensive psychiatric care would require 1,500,000 beds. The Central Inspection Board of the American Psychiatric Association found that twenty-nine mental hospitals had no psychiatrist at all; and that of the 300,000 registered nurses in the country, only 1,200 were directly involved in psychiatric nursing, even though 55 percent of all hospital beds were occupied by the mentally ill.
But the situation was even worse than just a resource problem. In an ideal world, professional physicians with credentials from the world’s best medical schools, and researchers who had tirelessly worked to decode the mysteries of the human brain, would work together to understand and treat the illnesses that kept patients in beds. But this isn’t what happened. Brain ‘science’ was still in an aspirational stage; despite the knowledge that had been collected, and despite the prestige of the many physicians dedicated to understanding mental illness, not much progress had been made. There were no cures and few treatments. People felt helpless and hopeless. As Valenstein says, “Almost any proposed treatment was considered worth trying, as long as it did not require much money or large numbers of skilled personnel.” (ch. 9, p. 177)
In such an environment, there is a very human urge to do something. If there is something that works sometimes, we should try it again. If our knowledge of the brain suggests something, we should try it. But if we have neither empirical success nor any theoretical ground to stand on, we still want to do something. And in the absence of strong safeguards, physicians seeking glory—and, to be fair to them, hoping to help the legions of sick patients, whose number only seemed to be growing as the years wore on—would simply try things. Sometimes these attempts were based on vague hunches about the brain, and sometimes they didn’t seem to be based on anything at all.
Acute demand inspired many dubious attempts to develop treatment. In Chapter 2, Valenstein focuses on three which were developed in the same decade, the 1930s, as the lobotomy: insulin coma, metrazol coma, and electroshock therapy. The last one is exactly what it sounds like (shock patients to deliberately induce seizures), and the first two literally involve deliberately putting patients into comas. The theoretical underpinnings of these therapies all seemed about the same. Maybe the brain is like a car engine or computer that doesn’t work: if you hit it a few times, then maybe it will reset and work better somehow. These therapies were dangerous and generally ineffective. (But more on electroshock therapy later.)
It must be emphasized that these treatments were not beyond the pale of normal medicine. They were normal medicine. Many similar treatments, which generally had little or no serious theoretical justification, were tried. Consider that Wagner-Jauregg’s treatment for neurosyphilis—which was to inject patients with malaria-infected blood to give them fevers, in the hopes that they could ‘sweat the illness out’—received the Nobel Prize in 1927!
(Incidentally, the treatment did work, although its fatality rate was high. The extreme fever killed or damaged the bacteria responsible for neurosyphilis. The malaria could then be treated with quinine.)
One of the worst ‘treatments’ was due to Henry Cotton, who thought that bacterial infections in the body caused mental illnesses: (ch. 2, p. 42)
We have estimated that about 80% of the so-called functional type of mental disorders are due not only to infected teeth and tonsils, but also to congenital malformations of the colon, or large intestines. …
… Relics of medical superstition and barbarism are being supplanted by up-to-date conceptions as to the true relation of structure and function. The inhuman neglect that has resulted from the old discredited philosophical dualism is being overcome by the idea of a unified mind and body.
It is extremely funny and sad that he thought his views supplanted “superstition and barbarism”.
The natural course of action, he thought, would be to remove infected parts of the body: teeth, the tonsils, parts of the cervix, parts of the colon, and more. The mortality rate for these procedures was extremely high (for colon resection, around 30 percent) and they obviously did not seriously help patients. I can’t imagine much worse than being extremely mentally ill, and then having a bunch of random body parts removed.
One dramatic therapy after another was tried and then mostly failed. This incentivized physicians seeking “fame and name” to try to make their mark by developing therapies which were still more dramatic. Perhaps what the treatment of mental illness needed was not conservatism, but even more daring.
IV. FAME AND NAME: THE CASE OF EGAS MONIZ
Egas Moniz was the kind of man who regularly exaggerated his accomplishments. Consider this anecdote: (ch. 11, p. 239)
Characteristically, Moniz, who had little musical talent, promoted the story that he had written a professionally staged operetta (actually a little at-home show with childhood friends).
He did it because he wanted recognition; he wanted to be viewed as smart, creative, and pioneering. Motivated by “fame and name” as much as anyone else has ever been, he became infamous for his 1935 invention of the prefrontal leucotomy, the precursor to the lobotomy.
Originally António Caetano de Abreu Freire, he was born in Avanca, Portugal in 1874. He was the eldest son of an aristocratic family that traced its lineage back to a twelfth-century folk hero named Egas Moniz who helped repel Moor invaders; “Egas Moniz” was added at to the end of his name at his christening, but as a boy he talked so much about the folk hero that people started calling him “Moniz”. Eventually, he just went by “Egas Moniz”, becoming the modern incarnation of the legendary hero.

Egas Moniz, the inventor of the prefrontal leucotomy.
Valenstein does not like Moniz, or at the very least thinks his fame-grubbing is kind of pathetic. He tries to correct the record wherever he can. For example, in a footnote he observes that: (ch. 4, p. 64)
It is characteristic of some of the myths surrounding Moniz’s life that the original Egas Moniz is described only as “a Portuguese patriot who roused the country to drive the Moors from the mountains of the Iberian peninsula.” Actually, the original Egas Moniz remained loyal to the House of Castille, representing Spanish domination, even though he was nominally in the service of Henrique, a nobleman who had assumed the title of king and led a rebellious movement for Portugal’s independence.
Moniz studied medicine at Coimbra University and was appointed a lecturer there after graduation. Later, he received neurology training in France. Two years after graduation, he published A Vida Sexual, a book which apparently includes “some of Freud’s revolutionary ideas on infant sexuality.” (ch. 4, p. 66)
Valenstein makes clear that Moniz was okay as a scientist and clinician, but much more gifted as a politician. He was elected to the Portuguese parliament (while keeping his position as lecturer) for the first time in 1900, just after graduating from medical school at Coimbra, and was repeatedly reelected. Valenstein says: (ch. 4, p. 66)
During this early period, he accomplished little of distinction in neurology. Indeed, when he was given the newly established professorship of neurology at the University of Lisbon in 1911, some colleagues at the university resented the appointment, considering it political rather than earned … Up to this time, his publications in neurology consisted of a few unfocused articles (mostly case reports) on “Jacksonian” epilepsy, encephalitis, and a thalamic pain syndrome.
Valenstein describes a book Moniz wrote around this time—on the neurology of traumatic war injuries—as “not an original contribution” with “little influence”. (ch. 4, p. 67)
Moniz’s political career was fairly successful. He helped negotiate concessions for Portugal after World War I ended and he was the dean of the University of Lisbon’s medical school for a time. He remained active in Portuguese politics and in Portugal’s parliament for years, and remained well-connected with a good reputation despite considerable political tumult. But his political aspirations petered out after a military coup in 1926, which a few years later led to the Salazar dictatorship.
Moniz was fifty-two then. By that time he had enjoyed a successful political career, had established a successful private practice, and had a middling career as an academic neurologist. Valenstein says that although some “would be content to rest on their laurels,” Moniz was dissatisfied: (ch. 4, p. 69)
… childless, embittered by politics, and dissatisfied with his accomplishments, he turned to neurology for both vindication and fulfillment.
So began a series of unfortunate events.
He met with his former mentor Jean Sicard in Paris. Sicard was experimenting with a kind of approach to visualizing organs; the hope is that, if internal organs can be visualized, it may be easier to diagnose patients, e.g., because a tumor can be more easily detected. Sicard was specifically doing this by injecting patients with opaque substances, which would then make organs visible under X rays.
Moniz decided to try to adapt the approach to visualize the brain. He began by experimenting with animals and cadavers: (ch. 4, p. 71)
Working under less than ideal conditions, Moniz injected the cadavers in the pathology department of the Institute of Anatomy and then transported the detached heads in his chauffeured limousine through the city streets to his laboratory in the Santa Marta Clinic, always fearing, as he later remarked, what would happen if a car accident revealed what he was carrying.
Satisfied with the fundamentals of the approach, he quickly began trying it on patients. His carelessness killed one patient and gave others neurological problems (like Horner syndrome), pain, or epileptic convulsions. But after several months, he finally obtained an adequate image (or cerebral angiograph) with his cerebral angiography technique. He immediately raced to Paris to “announce his discovery and establish his priority” (ch. 4, p. 72), although in Moniz’s telling he was unconcerned about such things and just so happened to have the angiograph handy when a relevant discussion took place during a meeting of the Neurological Society.
It was important for Moniz to establish that he deserved full credit for the idea, even if it was admittedly derivative of similar work going on at the time (and moreover was something others were already planning to do). Regarding Moniz’s race to receive credit, Valenstein writes: (ch. 4, p. 73)
Although the first useful picture from a patient had not been obtained until the end of June 1927, he had published 8 articles on the subject before the year ended, and 17 in 1928—a year in which he also made an extensive journey to Brazil to lecture on cerebral arteriography. By 1934, he had written 2 books and 112 articles on the subject.
Over the years, I’ve learned that it is sometimes best in academia not to be the most clever, but to be the most productive: publishing one hundred mediocre articles on a single idea may yield better results than publishing ten clever articles on distinct ideas. Many scholars have made a career out of being the X Person. If you’ve read about X, you’ve probably seen or heard about at least one of their approximately one hundred thousand articles on X. Given the above quote, I think Moniz would agree.
Moniz also actively sought recognition for his work: (ch. 4, p. 73-74)
According to the Medical Nobel Archives, early in 1928, less than six months after the first useful angiogram had been obtained, the Nobel Committee received two letters nominating Moniz for the prize in medicine. Both letters, dated January 1928, were sent by colleagues of his … at the University of Lisbon. The nominating letters were so brief—one consisting of only two sentences—that it is difficult to avoid the conclusion that they were written to fulfill an obligation, rather than out of any conviction.
He would also feud with others that, at least in his opinion, did not adequately cite his contributions. Even if his method was found to be dangerous and often unnecessary (on top of being rather derivative), he wanted credit.
In 1935, Moniz was sixty-one, and it was increasingly unlikely that he would receive the Nobel Prize for his cerebral angiography work, despite repeatedly getting his colleagues to nominate him. He had to find a new important problem to work on, and quickly—he was getting old.
At the Second International Congress of Neurology, in the August of 1935, something remarkable happened. During a symposium on the function of the frontal lobes of the brain, John Fulton and Carlyle Jacobsen from Yale reported some experiments they did with chimpanzees. These animals were trained to solve simple problems. One was a memory test which involved seeing a food treat placed under one of two cups, waiting some length of time (e.g., a few minutes) with the cups no longer visible, and then choosing the cup with the treat under it. Fulton and Jacobsen were interested in seeing what happens to their performance after much of their frontal lobes are destroyed, probably motivated by the idea that frontal lobes have something to do with ‘intelligence’ and ‘reasoning’ broadly construed.
One of the two chimpanzees had a tendency to have temper tantrums when she made a mistake. But after the surgery, she became serene. In other words, destruction of the frontal lobes produced a striking change in personality. According to Fulton, Moniz noticed this and asked about it after the presentation: (ch. 4, p. 78)
Dr. Moniz arose and asked if frontal lobe removal prevents the development of experimental neuroses in animals and eliminates frustrational behavior, why would it not be feasible to relieve anxiety states in man by surgical means?
At the time we were a little startled by the suggestion, for I thought that Dr. Moniz envisaged a bilateral lobectomy [removal of a large part of the frontal lobes on both sides of the brain], which though possible would be a very formidable undertaking in a human being.
Moniz got straight to work once he got home from London. He did not pilot experiments on animals; in collaboration with the surgeon Almeida Lima, he immediately began experimenting on humans. Characteristically, Moniz later denied that the International Congress presentation played any role in his decision to try treating mental illness via brain surgery. He claimed to have thought about it for several years before, and to have considerable theoretical backing for this idea; Valenstein argues at length that both claims are false. In brief, he thought it was feasible, and that if it worked it would make him famous.
In short order, Moniz and Almeida Lima found and operated on twenty patients. These patients varied in their illness—some had affective disorders like anxiety and depression, and others were schizophrenic. During this time, their procedure changed with each operation, sometimes considerably. While they initially damaged the frontal lobes by squirting alcohol into the brain through holes drilled in the skull, they later tried directly lesioning tissue with a sharp object they called the leucotome. Where they cut, how many cuts they used, and the construction of the leucotome also changed. Nonetheless, Moniz concluded that in the pilot cohort there were seven recoveries, seven improvements, and six patients that remained unchanged.
The prefrontal leucotomy was born.
(If at this point you’re wondering—who allowed this wanton experimentation on mentally ill patients?—keep in mind that modern institutional review boards did not exist, and there was no formal ethics review process.)
As in the case of cerebral angiography, Moniz raced to establish his priority. Less than four months after the first leucotomy operation, he wrote a monograph and article on these twenty cases, some of which had minimal followup. Moreover: (ch. 6, p. 113)
Before the end of 1936, Moniz had published essentially the same data in five more articles, in one of which he coined the term psychosurgery. … Thus, in a relatively brief period, Moniz had published articles on leucotomy in six different countries. Seven articles in addition to the monograph were published in 1936, and six more and a book appeared in 1937. Clearly, there could be no competing claims for the discovery. As Walter Freeman concluded, “Moniz was taking no chance of further piracy.”
Valenstein writes that this haste had a predictable downside: (ch. 6, p. 113)
Never in his monograph did Moniz seriously consider the possibility that any of the patients were worse after the operation. The six patients who did not improve were said simply to have been “unchanged” or “the same as before the operation.”
Although he did acknowledge and list many (serious) side effects, he claimed that they would eventually go away on their own. He argued bitterly with colleagues that were skeptical of the procedure.
Moniz’s contribution to the ‘science’ of psychosurgery more or less ended there, as he published no new articles on the leucotomy after 1937. This may have been in part due to poor health—Moniz became wheelchair-bound after a psychotic patient (albeit not one he had lobotomized!) shot him five times in 1939.
But his gambit paid off. A decade later, in 1949, Egas Moniz won the Nobel Prize in Physiology or Medicine. He shared the prize with Walter Hess, whose work had nothing to do with Moniz’s leucotomy or other kinds of psychosurgery.
Moniz’s story had something of a happy ending. He finally got the recognition he thought he deserved, even if it was built on poorly-supported claims and later harmed tens of thousands of patients. The nicest thing Valenstein has to say about him is this: (ch. 11, p. 239)
Born of another age, this "Renaissance man" had ... above all, a driving ambition to excel and to be recognized. … Though he was determined to be thought of as creative, within neurology he demonstrated little talent for delving into theoretical questions. Moniz made his mark by his ability to select and to solve important applied problems---not through innovation, but through trial and error, dogged persistence, and an uncommon willingness to take risks. Perhaps influenced by the idealized heroics of the great fifteenth-century Portuguese navigators, Moniz identified with and admired other great risk takers as well; in his dressing room in Avanca were three porcelain figures of Winston Churchill, born, like himself, in November 1874.
But Valenstein can’t help but add: (ch. 11, p. 239)
In his memoirs, Confidencias de um Investigador Cientifico, which reveal little about his inner thoughts and feelings, he quoted every word of every compliment he ever received from anyone of consequence. Even Walter Freeman, a great admirer of Moniz, was forced to write that "the book will particularly appeal to readers who have praised Egas Moniz, since they will find their words quoted in extenso."
The task of spreading and refining psychosurgery was left to others. Impressed by the importance of Moniz’s discovery, some took up this task with dogged determination.
V. FAME AND NAME: THE CASE OF WALTER FREEMAN
If Egas Moniz wrote the Old Testament of psychosurgery, Walter Freeman wrote the New Testament. If you subscribe to any flavor of the Great Man theory of history, he is The Man. Moniz may have ‘invented’ psychosurgery, but Freeman ‘perfected’ it. No man deserves more credit for its rise and infamy than him.
Depending on your perspective, he is either our story’s determined protagonist or its monstrous antagonist.
Walter Freeman, the inventor of the prefrontal lobotomy (with James Watts) and the most effective popularizer of psychosurgery.
Like Moniz, Walter Freeman came from a distinguished family and had a famous relative. His maternal grandfather was William Williams Keen, a leading surgeon and “one of the first brain surgeons in the United States.” (ch. 7, p. 122) Consider this episode from Keen’s career: (ch. 7, p. 123)
In 1893, for example, Keen had been summoned to remove the left side of President Grover Cleveland’s cancerous upper jaw—an operation undertaken in secret, so as not to add to the public’s nervousness during the financial crisis of that year.
His father was also a surgeon, although not one of any distinction.
Freeman was born in 1895 and enjoyed all of the usual benefits of growing up in a wealthy, educated family. He went to fancy private schools, grew up in a big house with servants, and was taught musical instruments and foreign languages. He went to Yale for his undergraduate degree, and then to the University of Pennsylvania for medical school in 1916 after deciding relatively late that medicine seemed more interesting than his other options.
As a medical student, he was driven and successful. It helped that his grandfather was a famous and well-connected surgeon: (ch. 7, p. 126)
… the summer before his senior year, Freeman worked at the Mayo Clinic—another position arranged by his grandfather, a close friend of William and Charles Mayo.
He decided to specialize in neurology and finished medical school in 1920. After a few years of internship, in 1923 he decided to spend time studying in Europe: (ch. 7, p. 127)
… a trip that, with his grandfather’s help and reputation, was not difficult to arrange. It was common at the time for young American neurologists who could afford it to spend a few years working in Europe. European neurologists were considered to be the intellectual leaders in the field, and time spent abroad could have practical advantages in securing desirable positions later …
He studied in Paris and Rome, where he used “crowbars and pickaxes” (ch. 7, p. 128) to extract the brain of a dead elephant for study. Freeman finished his tour in Vienna, and then returned to the United States in 1924 to work at St. Elizabeth’s Hospital. In short order, he also secured appointments at George Washington University (in neuropathology) and Georgetown University (in pathology).
Freeman was by this time a fully formed physician, but not yet a psychosurgery-obsessed menace. He was viewed fondly by his students, who considered him an engaging lecturer—especially compared with another professor, who apparently simply read from a textbook during his “lectures”. One students recalls his experience with Freeman as a teacher: (ch. 7, p. 132)
Dr. Walter Freeman, a goateed, hyperactive, flamboyant antiestablishmentarian, a brilliant eccentric, was professor of neurology at George Washington University. His classes in neurology were electric. His demonstrations of anatomy included on-the-spot dissections of the human brain, which he carried out with a small, sharp-pointed wooden stiletto, neatly demonstrating centers of brain cells and nerve pathways in moments. It would have taken others months to prepare them for demonstration. He drew diagrams upon the blackboard using both hands simultaneously to illustrate the anatomy of the nervous system … It was in his classes that I literally fell in love with the brain …
Remember the bit about Freeman being able to do something with both hands at once; that will come up again later. Valenstein adds: (ch. 7, p. 133)
Later these demonstrations became so popular that they were moved to the large “Hall A” auditorium of the Outpatient Clinic. Although they were held on Saturday and attendance was not required, there were often as many as seventy people in the room. Freeman was such a good performer that some of the medical students took their girlfriends along for the show.
Freeman’s successes continued apace. He was appointed a professor of neurology and head of his department in the fall of 1926 (at only thirty-one years old); he got married and had several kids (four by 1928, and eventually six in total); and using data he had already been collecting, he wrote a thesis and in 1931 obtained a PhD from Georgetown. He got ‘in’ with the American Medical Association (AMA) and became one of the examiners for a newly established certification board for neurology and psychiatry.
He was as eccentric as he was successful. His eventual partner in surgery, James Watts, recalled that he (ch. 7, p. 136)
… first saw Freeman in Atlantic City at the 1933 American Neurological Association meeting strutting down the boardwalk wearing a Texas sombrero and carrying a cane.
He was a carnival barker even at conferences, where he (ch. 7, p. 136)
… in order to draw a crowd, would call out that the show (short films he often made for a meeting) was just about to begin.
Freeman’s life was good but not perfect. He often overworked and overextended himself, which sometimes led to him harming patients. For example: (ch. 7, p. 135)
Curare and other muscle relaxants had not yet been developed to prevent the bone fractures often caused by shock treatment and Freeman would normally ask his secretary to help hold a patient down when he gave such treatment in his office. On one occasion, when he was treating a woman for depression, a new secretary refused to participate, so he proceeded alone. During the convulsion, the patient fractured the humerus bone in both arms. Freeman, who was late for an appointment in the hospital—with another patient—gave the woman an injection of morphine and left her in the office with her husband. When he returned, the woman had been writhing in pain for almost two hours. The husband was furious and contacted his lawyer immediately afterward.
He was entering middle age and listless: like Moniz, he was dissatisfied with how his life was going and searching for something to latch onto.
And then something remarkable happened. He attended the same 1935 International Congress of Neurology that Moniz did and met Moniz there. When he and his surgeon colleague James Watts stumbled onto Moniz’s first report on the leucotomy in early 1936, he became inspired. He swiftly ordered, read, and gave a glowing review to Moniz’s monograph. He called it “epoch making”. (ch. 8, p. 141)
He ordered leucotomes and, after practicing with Watts on cadaver brains, they prepared for the first operation on a real patient. They performed it on September 14th, 1936.
The prefrontal lobotomy was born. As Valenstein explains, Freeman and Watts chose the name because they thought the leucotomy label used by Moniz wasn’t accurate: (ch. 8, pp. 142-143)
Convinced that nerve-cell bodies as well as fibers were destroyed by the procedure, Freeman and Watts had decided on lobotomy as a more appropriate name for the operation than leucotomy, which implies the cutting of nerve fibers only.
In reality, their first operation had a questionable outcome (which we will discuss later). They did not perform much followup, but they were electrified by the result and rushed to write up and present the case. By November 18th, they had performed six operations and written up a report on them. In this early report, they note some caveats: (ch. 8, p. 143)
We wish to emphasize also that indiscriminate use of the procedure could result in vast harm. Prefrontal leucotomy should at present be reserved for a small group of specially selected cases in which conservative methods of treatment have not yielded satisfactory results.
This important warning was later disregarded by Freeman, who came to believe that operating before mental illness had progressed was essential for good results.
During a presentation of these results, Adolf Meyer, an ‘elder statesman’ of psychiatry, said: (ch. 8, p.144)
I should hesitate to promise that we could remove distraction and worries by operation. To call attention to what is possible might start an epidemic of hasty human experimentation.
But after stressing the need for a careful followup of psychosurgery patients, he added (ch. 8, p. 144):
… at the hands of Dr. Freeman and Watts, I know these conditions will be lived up to.
Ominous!
Freeman and Watts thought they were onto something, and pushed aggressively to do more operations to prove that their hunch was correct. But they increasingly appreciated that their results were mixed and inconsistent; for example, small changes in how far the instrument was pushed into the patient’s brain could produce large changes in outcomes. When many of their patients resumed their aberrant behavior after one lobotomy, they thought they ought to operate again, which greatly increased the risk of death and epileptic seizures. To address this issue, which provided ammo to their colleagues, in late 1937 they developed what came to be called the Freeman-Watts ‘standard’ lobotomy.
This involves some technical changes in how the procedure is done. But more importantly, they simply got more experience with it than Moniz ever did, which helped them learn the fine details of what ‘worked’. They found an interesting way to assess the success of their operations: (ch. 8, p. 151)
Having observed that the best therapeutic results seemed to occur when the lobotomy produced drowsiness and disorientation, Freeman and Watts began to use this “disorientation yardstick” to predict success. Whenever possible, they operated under local anesthesia, talking to the patient, asking questions, and getting the patient to perform tasks such as singing or subtracting sevens from one hundred. If they observed no signs of drowsiness or disorientation, they often destroyed a larger area. They reported observing that many anxious patients described a sudden reduction in psychic tension as the final cut was made.
Freeman and Watts continued doing procedures and promoting the lobotomy as a cure for all sorts of mental illnesses. They shifted their professional work to focus singlemindedly on it, and, leveraging their existing professional stature and Freeman’s successful attempts to court the press, positioned themselves as leaders of the field. They solidified their supremacy when their Psychosurgery: Intelligence, Emotion and Social Behavior Following Prefrontal Lobotomy for Mental Disorders was published in 1942.
Moniz’s monograph had quickly become outdated due to its narrow focus on Moniz and Lima’s early leucotomies, which did not even use a consistent procedure. Freeman and Watts’ Psychosurgery, meanwhile, reviewed a large volume of relevant literature and contained detailed discussion of surgical techniques and patient observations. It became the bible of lobotomies.
(If you like, Psychosurgery is the New Testament and Moniz’s more hastily written monograph is the Old Testament.)
I was curious to peek into the book, and found this strange passage on the first page of the Introduction:
There is, perhaps, something symbolic of the difference between East and West in the comparison of two notable modes of therapy, so effective at times and so opposite in conception, namely, psychoanalysis and psychosurgery. Contrast, for example, the passive mysticism of psychoanalysis, in its search for truth in the fundamentals of the developing personality, with the destructive surgical attack upon the brain in its attempt to relieve distressing symptoms. Continue the contrast, which is ever the greater between East and West, the present-day psychoanalysis originating in one of the eastern European capitals, Vienna, and psychosurgery in the most western, Lisbon. And finally, as to the fate of the originators, recall that the father of psychoanalysis died a Jew in exile and that the father of psychosurgery was shot (though not killed) by a homicidal maniac.
Also peculiar was the way the decidedly technical book was promoted. It was widely reviewed, even in venues which would not normally review similar books. In the New York Times, one reviewer wrote: (ch. 9, p. 171)
It is not too technical even for a layman … No novelist ever had a more thrilling subject.
Always the showman, Freeman designed the dust jacket and wrote the copy on the back of the book himself. One part of it reads: (ch. 9, p. 171)
Read the last chapter to find out how those treasured frontal lobes, supposed to be man’s most precious possession, can bring him to psychosis and suicide!
The jacket featured a foreboding illustration of a skull with black butterflies flying out of it. Valenstein says: (ch. 8, p. 165)
It was based on the French expression for feeling depressed: “J’ai des papillons noirs” (“I have black butterflies”). Freeman drew a skull with a trepanned hole from which black butterflies were emerging.
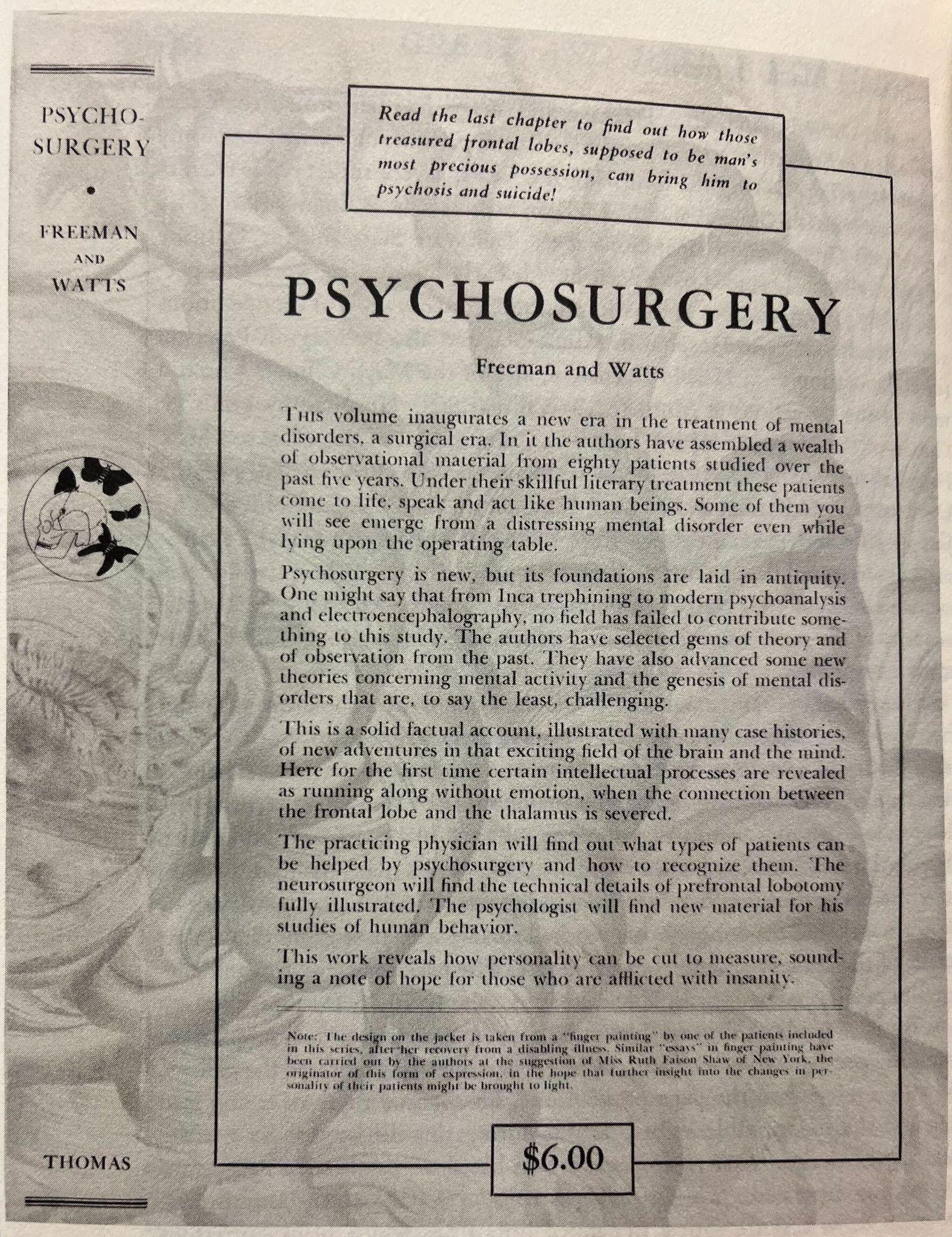
The cover of the first (1942) edition of Freeman and Watts’ Psychosurgery.

The skull on the cover. Note the black butterflies.
These were the golden years of Freeman and Watts’ collaboration. Together, they operated on hundreds of patients, and refined their version of the procedure. Freeman (somehow) became a media darling. The lobotomy became increasingly popular as a solution to the seemingly intractable problem of the legion of mentally ill patients, and was viewed as a lifeline for desperate families.
But then Freeman grew dissatisfied, again.
There were two problems. One is that the Freeman-Watts standard lobotomy could produce extremely deteriorated, apathetic patients, especially when patients were lobotomized more than once. (If at first you don’t succeed…) The second was that the Freeman-Watts lobotomy and its variants remained difficult and costly. It was a major surgery, and had both the expenses (i.e., it required neurosurgeons) and recovery considerations (weeks or months) associated with that. The crowded state hospitals usually had no neurosurgeon on staff because they were too expensive. There was simply too little funding, and too many patients, to pursue any large-scale lobotomy program. (Unfortunately!)
Freeman’s answer was what he called the transorbital lobotomy, which he conceived in 1945 and first started using on patients in early 1946. This version of the procedure adapted the approach Amarro Fiamberti used to access the brain: behind the eyeball, through the eye socket. It was lower-tech than the standard lobotomy because one did not need to drill holes through the skull. This came with the added benefits of (i) not requiring a neurosurgeon, and (ii) greatly reducing recovery time. Freeman envisioned training psychiatrists (generally with no experience doing brain surgery!) across the country to do the procedure, especially in state hospitals that could not previously ‘benefit’ from the lobotomy. He began a serious, yearslong campaign to realize this dream.
To prove the technique was ‘portable’, he performed the initial transorbital lobotomies in his office rather than in a hospital operating room. The first procedure used an ice pick from the Uline Ice Company. To show off, he would sometimes simultaneously manipulate two instruments inside a patient’s head at once, just as he had earlier written on blackboards with two hands at once in front of his students.
Many clinicians were horrified at Freeman’s new version of the lobotomy, despite the fact that most of them believed in the utility of the standard version. John Fulton wrote Freeman in disbelief: (ch. 10, p. 205)
What are these terrible things I hear about you doing lobotomies in your office with an ice pick? I have just been to California and Minnesota and heard about it in both places. Why not use a shotgun? It would be quicker!
Freeman’s reply included the quip: (ch. 10, p. 205)
It is much less traumatizing than a shotgun and almost as quick.
Freeman’s transorbital lobotomy was an abomination to neurosurgeons, who believed in strange practices like ‘using gloves’ and ‘draping the patient’. Valenstein elaborates on some of the fundamental conflicts: (ch. 13, p. 257)
Freeman was pitting transorbital lobotomy performed mainly by psychiatrists against prefrontal lobotomy performed by neurosurgeons. The resulting conflict was inevitable. Almost all neurosurgeons, Watts included, objected to transorbital lobotomy. They were appalled when they watched Freeman adjust the head straps for the electroconvulsive shock and then pick up the instruments with ungloved hands, and they resented the idea of inducing convulsions, which much of their work was aimed at eliminating. They were also concerned about the possibility of hemorrhage and infection. To neurosurgeons, transorbital lobotomy seemed to be a slapdash, hit-or-miss business, and the "assembly line" of operations on twenty or more patients in a row—averaging less than ten minutes each—a vulgar display.
Freeman, who did not himself have surgery privileges, as he was not a surgeon by training, should not have been doing the procedure alone. But he was doing them alone, because his usual partner-in-crime Watts (a neurosurgeon) could not accept the change. The productive Freeman and Watts partnership ended, and Freeman’s solo career began.
During the peak years of the lobotomy, which Valenstein identifies as between 1949 and 1952, Freeman spent a significant portion of his time on the road. He wanted to popularize his cheaper, faster transorbital approach, and chose to do so by visiting state hospitals across the United States (and sometimes elsewhere). Valenstein writes: (ch. 11, p. 229)
In 1951 alone, he visited hospitals in seventeen states as well as provincial hospitals in Canada. He also gave demonstrations in San Juan, Puerto Rico, and Willemstad, Curacao. On one five-week summer trip that year, he drove 11,0000 miles with a station wagon loaded, in addition to camping equipment, with an electroconvulsive shock box, a dictaphone, and a file cabinet filled with patient records, photographs, and correspondence; his surgical instruments were in his pocket.
He fastidiously kept track of the details of these trips. For example, he kept a list of the number of people he gave lobotomies and where he did them: (ch. 11, p. 230)
29 June, Little Rock, Arkansas, 4 patients
30 June, Rusk, Texas, 10 patients
1 July, Terrell, Texas, 7 patients
2 July, Wichita Falls, Texas, 3 patients
9 July, Patton, California, 5 patients
14 July, Berkeley, California, 3 patients
17 July, Mendocino, California, 9 patients
19 July, Fort Steilacoom, Washington, 7 patients
28 July, Sedro Woolley, Washington, 8 patients
4 August, Yankton, South Dakota, 5 patients
6 August, Lincoln, Nebraska, 8 patients
7 August, St. Joseph, Missouri, 1 patient
8 August, Cherokee, Iowa, 25 patients
9 August, Independence, Iowa, 16 patients
Note the last two dates: Freeman did twenty-five lobotomies in one day! Sometimes Freeman kept up this pace for a longer stretch. Valenstein notes that: (ch. 11, p. 234)
With the help of the staff at the hospitals in Lakin, Huntington, Spencer, and Easton, Freeman did 225 transorbital lobotomies during a twelve-day period in August 1952.
That’s around nineteen per day!
The schedule was grueling, from the long hours driving to the long hours doing surgery. Sometimes things went wrong; patients died. But Freeman remained committed to his vision. Thanks to his influence, more than half of all lobotomies performed in state hospitals were his transorbital version; elsewhere, the fraction was closer to 30 percent.
Like Moniz, Freeman sought recognition for his extreme efforts to advance psychosurgery. When Moniz asked Freeman if he could nominate him for the Nobel Prize—Moniz asked many people he knew, over many years, to do this—Freeman included a copy of his book with Watts with the nomination. Valenstein suggests that he might have been hoping to be considered with Moniz. After all, he and Watts were the faces of the field; their work ushered in a new era of lobotomy, and a new scale of worldwide usage.
Valenstein thinks he never had a chance, though: (ch. 11, p. 224)
Yet Freeman probably never had a chance to be nominated for the Nobel Prize. However effective he was at developing and improving ideas, he was not an initiator of new ones. Moreover, his habit of alienating people by his bluntness, self-assurance, and combative personality left a trail of opposition, if not enemies. Moniz, in contrast, was a paragon of tact.
Unlike Moniz, Freeman never got the prize. He also became increasingly alienated from the mainstream of neurology and psychiatry, both because of his combative personality and because he refused to adapt when times changed. Psychoactive drugs like chlorpromazine were widely adopted in the mid-1950s; this led to a precipitous decline in the usage of the comparatively riskier and more invasive lobotomy. But Freeman did not change. He was still doing transorbital lobotomies until his surgical privileges were taken away.
This happened when he killed his final patient, who was in the middle of receiving their third lobotomy from him: (ch. 14, p. 274)
He performed his last transorbital lobotomy at Herrick Memorial in February 1967, at the age of seventy-two. The patient was one of the ten transorbital lobotomies he had first performed in his office in Washington, D.C., in 1946. She had later moved to California; and, in 1956, Freeman had repeated the operation at Herrick. When, in this, the patient's third transorbital lobotomy, Freeman started to make the deep frontal cut, a blood vessel was ripped open, causing a severe internal hemorrhage. After the woman's death several hours later, his surgical privileges were taken away.
Freeman’s 1972 death was mostly ignored by the beleaguered psychosurgery community. He did achieve the fame he sought, but only temporarily.
VI. INTERLUDE: ABOUT THE LOBOTOMY
If you, like me, didn’t know much about lobotomy, you may have thought it was a generic term for surgical brain damage. It is more specific than that. But at the same time, it is much less specific than its proponents claimed. Its primary targets are the frontal lobes, which comprise a huge region of the brain. Moreover, as Freeman emphasizes in a 1950 journal article in the Journal of the National Medical Association:
Without entering into the minutiae of architectural patterns, it may be said that the major portion of the frontal lobe is of quite uniform architecture, and that the extent of incisions is of greater importance than their exact location.
This is almost certainly crazy and wrong, but it was the thinking at the time, at least among proponents of psychosurgery.
In any case, what is a lobotomy? There were several types.
The initial kind, the leucotomy developed by Moniz and Lima, had a few variants. They first tried destroying tissue by squirting alcohol through holes in the skull rather than by physically cutting the brain. Only after they had operated on a few patients did they begin physically cutting tissue, again through holes in the skull, using a sharp instrument they called a leucotome. The holes were usually drilled into the top of the skull.
The later Freeman-Watts ‘standard’ lobotomy continued using a leucotome to physically cut through tissue, but involved drilling holes into the sides of the skull rather than the top. Freeman and Watts found that this change helped them reduce variation in where they ended up cutting.
The third major type, the Lylerly-Poppens lobotomy, came to be preferred by neurosurgeons. Like the Moniz-Lima leucotomy, it involves accessing the skull from above, but uses larger openings made with the help of a long tweezers-like “speculum” tool. The larger openings made it effectively ‘open’, rather than ‘closed’: surgeons could see into the brain, which in principle allowed them to be more careful.
The final major kind, the transorbital lobotomy, was the low-tech version developed by Freeman. This one is the most different, since it involves drilling no holes through the skull. Instead, it involves pushing a sharp instrument through the bony orbit behind the eye, usually with the help of a mallet. (Imagine hammering a nail into someone’s head.) Freeman initially used the same leucotome he had used when doing standard lobotomies, but found that they had a propensity to break off inside people’s heads; this motivated him to construct a sturdier sharp object that he called an orbitoclast, which was around eight inches long and shaped like an ice pick.
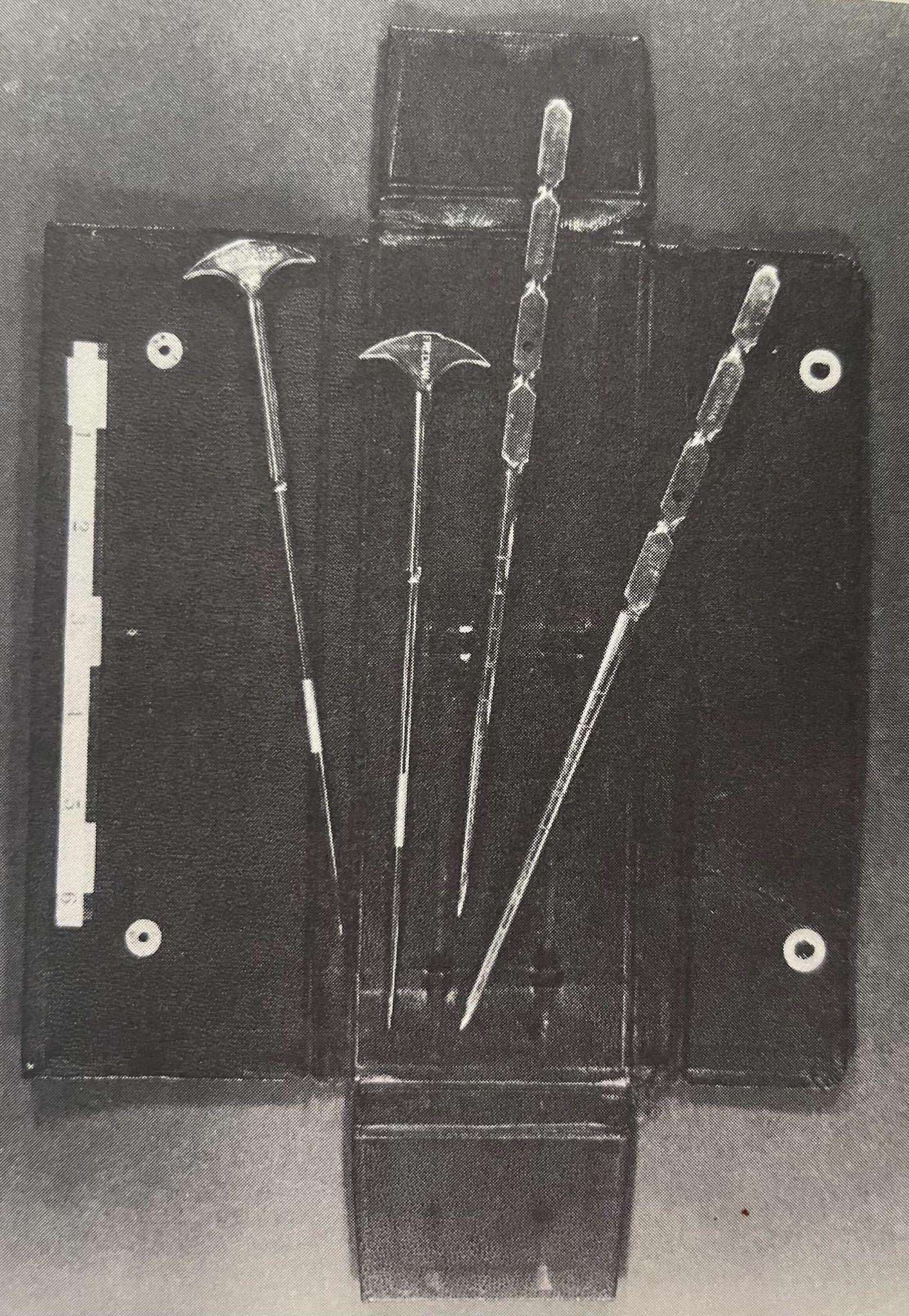
Freeman’s tools. As Valenstein says (ch. 11, p. 230), these are the “leucotomes and the orbitoclasts in the case that Freeman carried in the pocket of his suit jacket.”
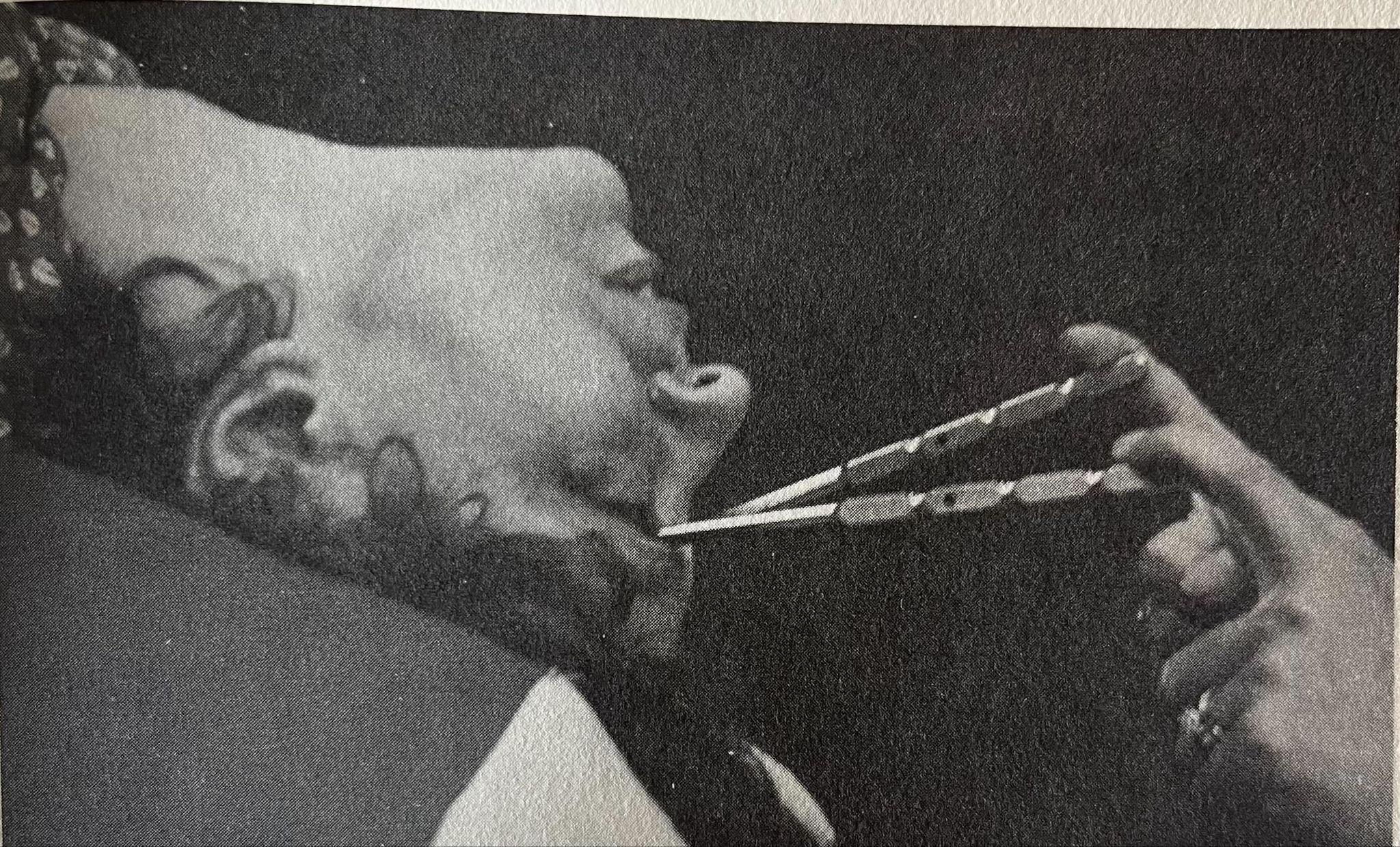
A transorbital lobotomy in progress. Note the orbitoclasts, which have been driven through the skull via the eye socket. Note also that Freeman is manipulating two of them at once.
The lobotomy was originally advertised as a method of last resort. As James Watts explained: (ch. 9, p. 183)
… patients with involutional or agitated depression with feelings of guilt who pace the floor, wringing their hands, mourning and crying. Still others with schizophrenia are confined to strong rooms because of their abusive assaultive behavior. If given a bed, they pull it apart and assault attendants with the pieces. They are often naked, refusing to wear clothes, urinate and defecate in the corner. … Food is poked through a crack in the door like feeding an animal in a cage. …
Following lobotomy, even the worst improve enough so that they live on an open ward, wear clothes, go to the dining room with other people, and get out in the sunshine.
Some members of the panel have suggested that we wait until they develop some form of therapy more to their liking. Perhaps I am a bit impatient at times. A woman 65 years old with agitated depression does not have but so long she can wait; and a man with dementia precox confined to a strong room for 5 years has already waited long enough.
But many of the tens of thousands of United States patients it was used on aren’t like those described in the above passage. Later, Freeman thought that the lobotomy should be used more liberally, since he thought that the outcome would be better before illness had progressed.
Valenstein positions his book as a history of psychosurgery rather than as a history of the lobotomy, probably for the reason that the lobotomy is a more specific term that does not describe everything that was tried. In the wake of the ‘success’ of the lobotomy, people tried targeting other brain regions, like the amygdala and other targets within the temporal lobes. These other operations had different results, but did not substantially differ in their ability to successfully treat mental illness—that is, they mostly didn’t work.
VII. INTERLUDE: CONSEQUENCES OF LOBOTOMY
Not all people that got lobotomies became zombies. Freeman bragged about patients who were ‘success stories’: (ch. 14, p. 282)
… a psychiatrist who, after a transorbital lobotomy, had become chief of clinical service in his own private clinic; another lobotomized physician who had subsequently married, had children, established a ten-man medical clinic, and flew his own plane; a violinist in a metropolitan symphony orchestra; and a college graduate who had become chief construction engineer for a major corporation.
Who says lobotomized people can’t be good pilots?
But these patients were of course not representative. Most lobotomized patients developed serious deficits: they became unmotivated, dull, and lacking in judgment. And these are the ‘good’ outcomes. Many patients simply died, further deteriorated, or developed serious epileptic seizures. As a superintendent of one state hospital said, (ch. 13, p. 255)
I am sorry to say that even when they improved they are nothing to brag about. ... These patients have not been completely restored and some of their families are extremely disappointed.
Or as the director of a major psychiatric institute said: (ch. 13, p. 255)
Is the quieting of the patient a cure? Perhaps all it accomplishes is to make things more convenient for the people who have to nurse them. ... The patients become rather childlike. ... They act like they have been hit over the head with a club and are as dull as blazes. ... It disturbs me to see the number of zombies that these operations turn out. I would guess that lobotomies going on all over the world have caused more mental invalids than they've cured. ... I think it should be stopped before we dement too large a section of the population.
The “zombie” assessment was sometimes fair, but the overall outlook was more complicated. Valenstein thinks: (ch. 12, p. 252)
Following a lobotomy, many agitated and anxious patients did experience a striking relief from their most troublesome symptoms. In the best cases, this led to a normalization of their behavior. In the worst cases, they became either thoughtlessly impulsive or almost insert, seldom talking and completely lacking in spontaneity. The latter cases justified the accusation that lobotomies were producing "zombies." Some patients became careless, indifferent to errors, and generally slovenly. Motivation and drive were often decreased, as were insight and foresight. Behavior tended to be more concrete, and patients were less capable of dealing with abstract ideas.
Part of the problem was that the ‘effectiveness’ of the lobotomy depended strongly on the patient’s illness. Over time, Freeman found that it did not do much for schizophrenics, but sort of worked on patients with affective disorders (e.g., extreme anxiety) since it could ‘flatten out’ their emotions.
Valenstein discusses a number of patient outcomes in the book. First, there are the historically significant patients, like the ones who Moniz and Lima or Freeman and Watts first operated on. Apparently Freeman and Watts’ first patient had this to say after her lobotomy: (ch. 8, p. 142)
FREEMAN: “Are you happy?”
PATIENT: “Yes.”
FREEMAN: “Do you remember being upset when you came here?”
PATIENT: “Yes, I was quite upset, wasn’t I?”
FREEMAN: “What was it all about?”
PATIENT: “I don’t know. I seem to have forgotten. It doesn’t seem important now.”
He adds ominously that “She greeted her husband with a peaceful smile.” This outcome was so encouraging that it caused Freeman and Watts to rush ahead with doing more lobotomies and quickly publish their results.
Then there are patients whose long-term study allowed Valenstein to discuss their outcomes in more detail. In Chapter 12, he considers two such patients, who are known by the pseudonyms Carolyn W. and J.S.
Carolyn W. was the daughter of a wealthy family who had a psychotic break after her parents, who didn’t approve of her marriage, had it annulled against her wishes. She became psychotic and suicidal, and had to be moved to a private sanatorium for care. Her doctors tried everything, with no success: (ch. 12, p. 243)
She was given all the available therapies for schizophrenia, including insulin coma, electroshock treatment, sedatives (antipsychotic drugs were still in the future), hydrotherapy, and wet packs; when there was a danger she would injure herself, she was placed in seclusion, sometimes in a straitjacket for restraint. No treatment produced any lasting improvement.
Other options having been exhausted, it was eventually suggested that she should have a standard Freeman-Watts lobotomy. This didn’t work, so (if at first you don’t succeed…) she was given a second, ‘radical’ prefrontal lobotomy, which involved more cutting than the original version. Unsurprisingly, this operation “markedly subdued” Carolyn and made her childlike: (ch. 12, p. 244)
Initially, the job was almost like caring for a child; Carolyn had to be brought to the bathroom and essentially toilet-trained. It was also necessary to supervise all her routine activities, even dressing, eating, and bathing. She seemed to be indifferent to pain and once stepped into scalding bath water, severely burning her foot. Like many of the early lobotomized patients, she had bulimia and ate voraciously: it is believed that the frontal lobes normally suppress "lower centers" in the hypothalamus and other areas in the brain that stimulate appetite; following destruction of the frontal lobes, or its exiting fibers, it was not uncommon for patients to gain more than fifty pounds. She also had a tendency to start fires in her room during the first six months after her discharge from the hospital.
What an ending!
Her family’s wealth enabled her to receive the highest levels of care in the years since her operation. She was not kept idle, but constantly given lessons, taken on trips, and otherwise stimulated. While this produced some improvement, (ch. 12, p. 244)
… she is not able to take care of herself and has required full-time caretakers. She is usually able to verbalize what she should do, but there is no guarantee that she will do it. Even though she could state what bus she should take to get to her art teacher, Carolyn took the first bus that came along and had to be rescued at different locations around the city when she was given several opportunities to make the trip alone. She is now always accompanied when she travels.
One of the weirdest things about Carolyn W. and other lobotomy patients is that their IQs are not necessarily low: hers is between 115 and 120. Valenstein says that “people meeting her for the first time usually do not detect any abnormality and consider her a proper, affable, well dressed, and somewhat taciturn lady.” (ch. 12, p. 245) But she clearly has major deficits, and these become obvious to anyone that spends more time around her.
It is apparently difficult to quantify these deficits in psychological tests, despite the fact that these patients exhibit horrendous judgment and require full-time caretakers. The results of IQ tests come out in the normal-to-bright range, and so do the results of many similar tests. One that Carolyn W. apparently struggles with is the Wisconsin Card Sorting Test, which measures “flexibility in thinking”. The subject originally sorts cards depicting some number of colored shapes (e.g., two red triangles) according to one feature, like shape, and then later is asked to switch to sorting based on a different feature. Patients like Carolyn have a hard time shifting strategies. This seems to accord reasonably well with what is known about the prefrontal cortex’s role in accommodating context information during context-sensitive decisions.
Muddying the waters a bit is that Valenstein doesn’t seem to be sure that all of Carolyn’s deficits are due to her (two!) lobotomies, since she also spent considerable time in an institution and received many other dangerous therapies: (ch. 12, p. 246)
Her limitations make it easy to criticize those responsible for the decision to perform the lobotomies. At the time, however, most psychiatrists considered it almost a certainty that any schizophrenic patient hospitalized for more than ten years would only deteriorate further. Carolyn seemed destined to spend her remaining years locked in a mental institution. Today, we might wonder whether some of her limitations were not the result of fourteen years of confinement in a mental institution where more electroconvulsive shock was surely administered than would now be considered safe.
But overall, Valenstein thinks Carolyn’s outcome, which has reduced her to a dull, dependent, childlike woman, is relatively good. Without the constant enrichment in the years following her operation, she likely would have become worse.
He contrasts her case with that of J.S., a sexual deviant who received a lobotomy after going to prison for sex crimes. He lived with his mother and had an Oedipus complex par excellence: (ch. 12, p. 247)
J.S. thought he had been spoiled as a child. He was very fond of his mother even though she was strong-willed and domineering. She had punished him physically for the slightest offense, beating him "with a strap, or birch switch, or with her hands on his bare buttocks." These beatings usually produced an erection and often ended with J.S. ejaculating and his mother kissing him. This behavior continued for about two or three times a week until he was sixteen.
Later, he became obsessed with the pleasure he derived from the beatings he had received as a child, and tried to get others to help him act out his sexual fantasies. Since people his own age wouldn’t help, he started trying to get children involved: (ch. 12, pp. 247-248)
His strategy was to start talking to young boys and quickly direct the conversation to questions about how their parents punished them. He would tell them that he liked it when he was beaten as a boy, and would make up a game where the boys acted as his parents and would have to punish him.
This escalated in a predictable bad way, and he was caught and imprisoned. In prison, he became obsessed with the idea that his obsession would lead him to commit even worse sexual and violent acts. J.S.’s high anxiety surrounding this is what led his psychiatrist to seek a lobotomy for him. The outcome did not initially seem good, but later improved: (ch. 12, pp. 248-249)
Immediately afterward, J.S. was confused, disoriented, and incontinent. He masturbated and kept placing his finger in his rectum and then in his mouth. After several days, however, he regained control of his anal sphincter; and by the tenth postoperative day, the confusion was said to have completely cleared up. Two to three weeks after the operation, all of the undesirable effects were said to have disappeared entirely. Although J.S. remained under observation in the prison hospital for six months, he was able to resume secretarial duties throughout most of this period.
Later, a journal article championed him as an example of the positive effects of the lobotomy. He was considered reformed, and gave a statement recanting his past deviant behavior. In 1942, one year after his lobotomy, he was released from prison.
He seemed to be on good behavior for a while, and regularly reported to his parole officer, but in 1944 stopped contacting him after he moved to Chicago. Then things got much worse: (ch. 12, p. 250)
Shortly after the lobotomy, J.S. appeared to have undergone rapid improvement, followed by a year-long period of stabilization and then a period of progressive decline. He was not able to hold a job for more than a few weeks before he was fired, because he was "undependable in every way" and did not seem "to know what he was doing." His judgment was childish, he had no insight into his behavior, and he became progressively confused. His memory was very bad, and almost nothing he said about previous events was found, when checked, to be accurate. He was often incontinent, and his buttocks were grossly contaminated with fecal matter. He exuded a profound stench and was covered with bedbug sores.
Even worse, he was still a pedophile, albeit an extremely incompetent one: (ch. 12, p. 250)
Earlier, the parole officer had given J.S. "a clean slate," reporting that he was "completely free of abnormal desires." In actuality, J.S. continued secretly to practice his perversions in Chicago. In his suitcase were found obscene handwritten propositions on slips of paper, which he handed out to boys in the parks he frequented.
Valenstein thinks that J.S. suffered from at least two problems. First, the lobotomy did not remove the obsessional desires that were consuming him, even if they apparently briefly quieted them. Second, lobotomized patients, which generally lacked the good judgment and mental adeptness to make it in the world without significant help, should not be left to their own devices. J.S. should have received some form of support in order to avoid relapsing and deteriorating.
Valenstein’s overall conclusion is that lobotomized patients were generally semi-competent, and in the best cases could get by with social support and by compensating for what they had lost: (ch. 12, p. 252)
In most cases, the impairment was at some intermediate level. Thus, there was some helpful reduction in the most troublesome symptoms—but at the price of reducing potential motivation to excel and the capacity for thinking abstractly, for imagination, for emotional experience, for spontaneity, for planning ability, for insight, and for social judgment. In the best cases, these deficits were not great, and, postoperatively, patients could make a good adjustment by compensating for the loss by using remaining abilities resourcefully, much as some elderly people are capable of doing.
But overall, he unsurprisingly does not think that the benefits of the lobotomy outweighed the risks, especially when it was not used as a method of last resort.
It is worth keeping in mind how dangerous the operation is. Death wasn’t uncommon. In one harrowing incident during one of Freeman’s road trips: (ch. 11, p. 231)
On the 1951 trip, there were four deaths from the surgery. The experience at the Cherokee State Hospital in Iowa was the worst: three of the twenty-five patients died either during or shortly after surgery. Two deaths were caused by hemorrhage, and one by an accident that caught Freeman completely by surprise. Normally it took a certain force to drive the leucotome through the bony orbit, but in this patient, the bone was so thin that the leucotome went through with hardly a touch from the mallet. When Freeman, as was his custom, stepped back to photograph the leucotome in place, it sank a full two inches farther into the brain up to the hilt of the handle. This patient never regained consciousness; and when the brain was later autopsied, the tip was found to have gone far beyond the frontal lobes, extending deep into the midbrain: indeed, the tip had penetrated the basal ganglia, skirting the hypothalamus and ending near the red nucleus.
In other words, a patient died because Freeman stopped to take a picture. Valenstein goes on: (ch. 11, p. 231)
Freeman would not allow himself to be emotionally drained by guilt when things went wrong. He had the attitude of a general conducting a military campaign: losses would have to be incurred on the way to ultimate victory.
This attitude drove many proponents of psychosurgery to continue even in the face of many middling and poor results.
VIII. UNCRITICAL RESEARCHERS
The peak years of psychosurgery occurred before we had good, widely-used models of how neurons in the brain process information, and before we had any serious knowledge of molecular biology. We were still in something of a dark age of neuroscience.
There was no agreed-upon way of thinking about the brain, so many different ways coexisted. And some of them were extremely strange. A particularly weird episode of the book involves the critique a Freudian psychoanalyst has of lobotomies. He thinks everyone should be aware that the compulsions associated with some mental illnesses (obviously) relate to an anal sensory perception area: (ch. 9, p. 183)
If we accept the general Freudian formula, and I see no reason not to, then the compulsion neurosis uses the mechanism of displacement from early erotic fixations. … Psychoanalytic psychiatry has pointed very clearly to a highly important organ libido investment in the “compulsion neurosis.” This is the cathexis of the anal sadistic with its massive hostility drive. This anal sensory perception elaborating area, Dr. Penfield I think partly localized at our 1934 meeting.
The (obvious) consequence of this is that lobotomies can only be successful if they sever “only the fibers connecting the frontal lobe with the brain area that receives sensory information from the anus”. (ch. 9, p. 184) These comments are so weird that a different prominent psychoanalyst feels compelled to speak against them: (ch. 9, p. 184)
I cannot understand why such ideas are brought here, and much less the fantastic conclusions drawn from them by some of the discussers. I suppose we are so polite that anything may be ventured with impunity. … The whole presentation reminds me of a time when they used to treat homosexuality by prostatic massage. … I asked him how he expected to cure homosexuality by prostatic massage. He thought the massage might rub out the homosexual cells and that they would be replaced by heterosexual cells …
Ouch!
Anyway, that was the state of some discussions of the brain: “anything may be ventured with impunity.” Valenstein asks: given this deep and substantial ignorance of the brain, should the proponents of psychosurgery have known better? He argues that the answer is yes.
First, even then a nontrivial amount of information was known about the anatomy and function of the frontal lobes. Valenstein points out that, in 1861 or possibly earlier, Pierre Paul Broca (of Broca’s area fame) thought that the frontal lobes had something to do with Man’s “higher faculties”: (ch. 5, p. 89)
The majesty of the human being is owing to the superior faculties which do not exist or are very rudimentary in all other animals; judgment, comparison, reflection, invention, and above all the faculty of abstraction, exist in man only. The whole of these higher faculties constitute the intellect, or, properly called, understanding, and it is this part of the cerebral functions that we place in the anterior lobes of the brain.
Work by many others, from then until the dawn of psychosurgery during the following century, established that the frontal lobes mostly consisted of neither sensory nor motor areas, but something else related to abstraction and problem-solving—and for this reason, the frontal lobes were sometimes called “association” areas.
The story of Phineas Gage, the construction foreman whose frontal lobes were severely damaged by a long tamping rod after an accidental explosion, was well-known. He exhibited severe deficits, including poor judgment and self-control. Moreover, similar deficits were observed in World War I veterans whose frontal lobes had been damaged.
It was known, but perhaps not widely appreciated, that patients whose frontal lobes had been deliberately damaged during surgery (e.g., to remove a tumor) also exhibited serious deficits. Moniz, who explicitly referenced some of these patients in his writings, apparently did not understand or ignored the severity of these deficits. He ought to have known that frontal lobe damage was likely to destroy something precious to human intelligence.
Valenstein’s other points concern the nature of the empirical evidence. The N = 2 chimpanzee study presented by John Fulton and Carlyle Jacobsen at the 1935 International Congress of Neurology was frequently either accidentally or fraudulently misrepresented, especially by Moniz. Moniz and others—including Fulton!—often claimed that both animals became more placid and agreeable after surgery. But this is exactly the opposite of what happened. One of them did—Jacobsen described the change by saying it is as if she joined a “happiness cult” (ch. 5, p. 96)—but the other one experienced the complete opposite trajectory! The other animal, who initially performed well, began making many errors and became prone to having temper tantrums. At least for her, damaging the frontal lobes created a kind of personality issue. Hence, the Fulton-Jacobsen study provided no evidence that frontal lobe damage reduces or eliminates neuroses.
As Valenstein observes, even the Nobel Committee made this error: (ch. 13, pp. 266-267)
Fulton's repeated distortion of the chimpanzee experiment came to be so widely accepted that when the Nobel Committee, in their citation of Moniz's award, traced the lines of thought that led to the discovery of prefrontal leucotomy, they perpetuated this error …
Valenstein rips apart Moniz’s ‘theoretical’ motivation for psychosurgery in a chapter aptly titled “The Emperor’s New Clothes: Moniz’s Theoretical Justification for Psychosurgery”. The first funny part of this chapter is that Moniz apparently had a history of lying about his justification for trying psychosurgery. Since, even then, using sharp objects to cut through people’s brains seemed a bit cavalier, especially in the absence of a concrete reason like a tumor, Moniz claimed that he had thought very hard about the whole thing. He had thought for years and had strong theoretical reasons to do what he did.
But that was a complete fabrication!
He claimed to have secret discussions with collaborators, but there is no written record of these discussions, and these collaborators could not remember them when asked years later. As Valenstein observes, you would think that they would remember them given the later infamy of psychosurgery. When he did disclose his theoretical motivation, long after the first operations had been done, it was pretty shallow. Valenstein calls it “not much of a theory at all”. (ch. 5, p. 84) It went something like this: (ch. 5, p. 84)
Moniz’s argument for prefrontal leucotomy was based solely on a series of general, loosely connected, and essentially untestable statements. First, he asserted that the frontal lobes are the seat of man’s “psychic activity,” and that thoughts and ideas are somehow stored in the nerve-fiber connections between brain cells. Moniz then stated that all serious mental disorders are the result of “fixed” thoughts that interfere with normal mental life. … Moniz argued that “fixed thoughts” are maintained by nerve pathways in the frontal lobes which have become pathologically “fixed” or “stabilized”. Effective therapy, according to Moniz, required the destruction of these abnormally “stabilized” pathways in the frontal lobes.
Among other problems, “fixed” thought patterns are a problem in some mental illnesses (like hysteria) but not others. And even if Moniz were right, it doesn’t follow that an untargeted operation involving sticking a knife into someone’s brain will address the problematic patterns!
Many of the early pioneers of psychosurgery expressed reservations with Moniz’s ideas, and were mainly motivated by (what they viewed to be) the empirically good outcomes. When Freeman and Watts published the first edition of their psychosurgery bible in 1942, part of what they offered was an alternative, more acceptable explanation for why psychosurgery ‘worked’, which helped others become more comfortable with it. As Valenstein explains, (ch. 9, p. 171)
What was most influential in Psychosurgery, however, was the theory that specific brain pathways between the frontal lobes and the thalamus regulate the intensity of the emotions invested in ideas. This was widely and uncritically accepted as the most promising scientific justification for psychosurgery.
Explaining its ‘success’ in terms of specific anatomical connections seemed at least more respectable than Moniz’s ‘fixed ideas’ framework. Still, like Moniz’s hypothesis, Freeman and Watts’ hypothesis has obvious problems: for one, not every serious mental illness they treated using psychosurgery involved intensely dysregulated emotions.
But perhaps these researchers and clinicians can be forgiven for not understanding the brain back in the 1940s. Their more serious, avoidable error concerned their liberal interpretation of experimental results. The twenty patients Moniz discussed in his original monograph did not provide good evidence that psychosurgery was effective. As Valenstein notes, (ch. 6, p. 108)
In four of the seven “cured” patients, the last observation Moniz recorded in the monograph was less than eleven days after the operation!
Additionally, the information collected and provided about patient outcomes seems to have been fairly limited. No quantitative tests were administered and no detailed notes were taken; only brief observations by a psychiatrist, which were from not long after the surgery, were included. The evidence base Moniz presented was totally inadequate, especially given the obvious dangers of brain surgery.
Worst, influential neurologists and psychiatrists like John Fulton of Yale began to uncritically repeat the claim that Moniz’s evidence base was solid. This seems to be a case of someone saying it once, and then everyone else repeating it without ever actually reading Moniz’s book.
Later, Freeman was more scrupulous about following up with his patients, even after many years. But Freeman also did not usually administer psychological tests and was probably too invested in the success of his procedures. He tried to report outcomes honestly, but he also saw what he wanted to see; confirmation bias was a huge issue.
Given the sorry initial state of many of the patients who underwent psychosurgery, it was hard for physicians to assess outcomes. If someone who was initially violent and incoherent became dull and placid, and at the very least no longer needed to be restrained, did that count as an improvement? The experimental evidence was hard to evaluate, and there did not seem to be any large-scale attempt to compare outcomes to those of an appropriate control group.
There are two final interesting ingredients worth mentioning. One is that Moniz and Freeman were both respected senior researchers and physicians when they began psychosurgery; this helped insulate them from criticism. Influential senior people spoke up for them and repeatedly gave them the benefit of the doubt, even when what they were doing was poorly motivated and sometimes crazy.
The other was a tendency toward incremental change. When people criticized psychosurgery, especially once it became popular and widespread, it was not on its fundamentals—rather, it was on the details of an approach. It was assumed that if it was ever ineffective, the fix was to refine and improve the procedure rather than to abandon it entirely. This situation makes me imagine some exchange like this:
PERSON A: Maybe we should blow up the entire world.
PERSON B: That’s preposterous. We need to be extremely careful. What if we just blew up 99% of the world?
Once psychosurgery gained momentum, it was hard to get rid of it entirely. People were too invested in it and had too many ideas about how to ‘get it to work’. In some sense we are lucky that psychoactive drugs came when they did and worked as well as they did. Otherwise, we may have been stuck toying with psychosurgery approaches for much longer.
IX. UNCRITICAL MEDIA
For years, I’ve read and enjoyed blogs like Not Even Wrong and Shtetl-Optimized. It’s fun to see educated bloggers take down outrageous claims like ‘physicists find evidence for the multiverse’ or ‘physicists create a black hole on a tabletop’ or whatever. (For whatever reason, this happens a lot with theoretical physics.)
But it’s one thing when the hype machine boosts speculative theoretical physics claims that have nothing to do with everyday life. It is an entirely different thing when what is being hyped is a miracle cure to your most serious problems.
Part of Valenstein’s argument is that, thanks to the efforts of people like Freeman, and also thanks to people’s natural tendency to be optimistic that miracle cures actually work (see, e.g., Dr. Oz and similar old daytime shows), the media uncritically promoted psychosurgery before it could be properly vetted. This is obviously bad: journalists were in no position to evaluate the complex evidence that bore on the question of whether psychosurgery was justified, and the coverage provided laypeople with an unrealistic picture of the costs and benefits of the procedure. The whole media circus increased demand, and the optimism surrounding it partly silenced voices critical of psychosurgery.
The atmosphere of the times might be summarized by this October 1949 quote from the New York Times: (ch. 11, p. 221)
Hypochondriacs no longer thought they were going to die, would-be suicides found life acceptable, sufferers from persecution complex forgot the machinations of imaginary conspirators. Prefrontal lobotomy, as the operation is called, was made possible by the localization of fears, hates and instincts. It is fitting, then, that the Nobel Prize in medicine should be shared by Hess and Moniz. Surgeons now think no more of operations on the brain than they do of removing an appendix.
Needless to say, surgeons do not and should not think that!!!
Here’s a selection of fawning small-town newspaper headlines Valenstein lists on p. 157:
SURGEON’S KNIFE RESTORES SANITY TO NERVE VICTIMS
WIZARDRY OF SURGERY RESTORES SANITY TO FIFTY RAVING MANIACS
BRAIN SURGERY IS CREDITED WITH CURE OF 50 HOPELESSLY INSANE
FORGETTING OPERATION BLEACHES BRAIN
NO WORSE THAN REMOVING TOOTH
Life magazine ran articles filled with whimsical cartoons whose goal was to explain the lobotomy. This one explained it in terms of the Freudian concepts of the id, ego, and superego:
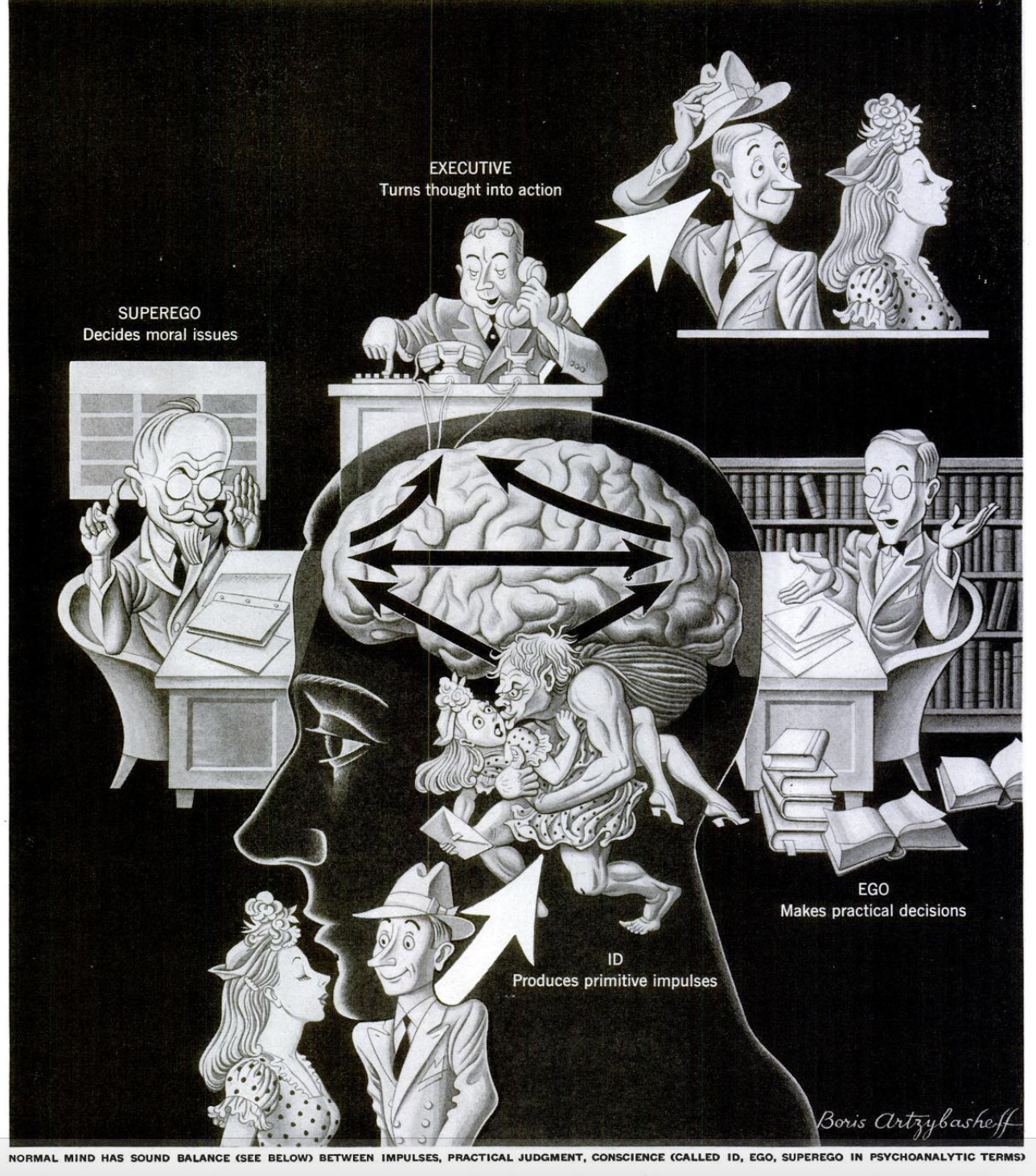
From the March 3, 1947 issue of Life. In a healthy man, the various Freudian sub-entities are harmoniously balanced.
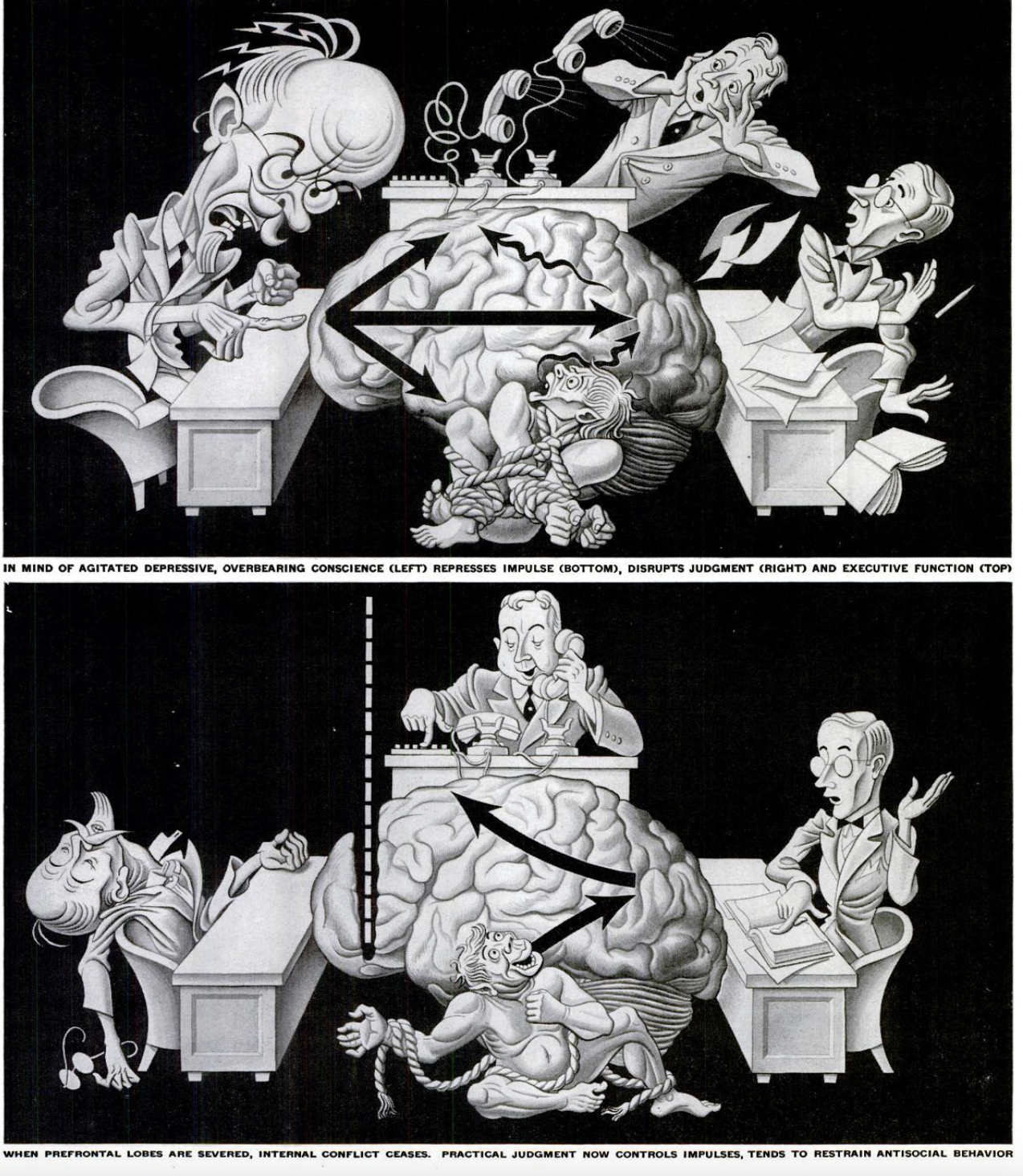
From the March 3, 1947 issue of Life. In a mentally ill man, the superego is out of control! They claim that the lobotomy makes him shut up. But I’m not sure where they got this explanation from.
Side note, the same article also depicts graphic images of brain surgery next to an ad for shoes:
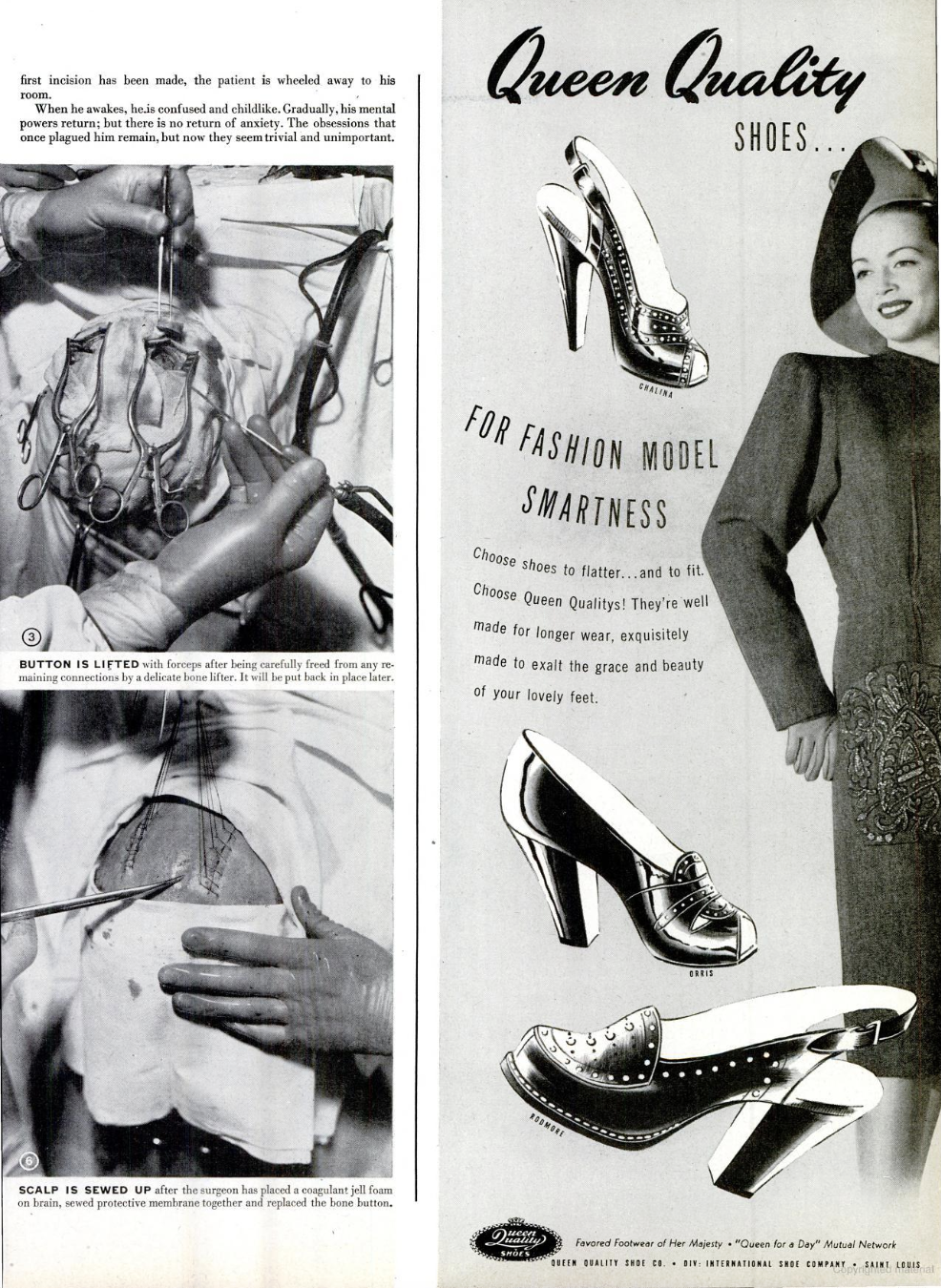
Get yourself a magazine that can do both.
Different popular accounts of the lobotomy were not generally consistent with one another: (ch. 9, p. 180)
Thus, while Life described the effects of lobotomy as destroying the superego, Time implied that the operation created a superego where apparently there had been none before.
The hype was also not limited to media aimed at laypeople. Even the prestigious New England Journal of Medicine joined in: (ch. 10, p. 199)
A new psychiatry may be said to have been born in 1935, when Moniz took his first bold step.
Or consider a 1941 editorial in the Journal of the American Medical Association, another ‘establishment’ publication: (ch. 9, p. 187)
An emotional attitude of violent unreasoning opposition to this form of treatment [lobotomy] would be inexcusable. True it is a mutilating operation and it does result in certain defects in personality and behavior. However, much surgery is mutilating in the sense that some ordinary normal tissue is removed in order to achieve a beneficial result. … No doctor can yet assert that this is or is not a truly worthwhile procedure. The ultimate decision must await the production of more scientific evidence.
And of course, the Nobel Prize was the biggest rubber stamp of all!
A substantial chunk of this hype was either encouraged by or directly produced by Freeman, who had a penchant for showmanship and a love for the limelight. For example, Freeman and Watts maintained a “psychosurgery exhibit” in the exhibit hall of the American Medical Association’s annual meeting from 1936 to 1946, the prime years of their collaboration. Watts recalled that: (ch. 8, p. 160)
He would stand by his exhibit, and as people approached, he had a clicker which made a sharp staccato noise. When they stopped he would begin to talk like a barker at a carnival. Then a crowd would gather and before they moved on they had heard the story of dramatic relief of emotional tension, depression, suicidal ideas, had seen pre- and post-operative photographs, x-rays and sketches of the lobotomy operation.
Freeman didn’t care if his fellow physicians found his approach—that is, the enthusiastic promotion of a dangerous and incompletely understood brain surgery—distasteful. He blamed his colleagues for being unfair, and spun his behavior as being due to a concern for patients’ wellbeing: (ch. 8, p. 161)
When it is a question of overcoming inertia and taking part in the pressure of the public upon politicians, and particularly upon hospital administrators at least to give the method described a fair trial, then I think that the doctor with a clear conscience can discuss his research with newspaper reporters and undergo the ensuing censure from his colleagues with equanimity. He realizes that something is being done to apply his discovery to the welfare of suffering patients.
With the media portraying brain surgery as ‘trendy’, even famous and wealthy people sought lobotomies for their families, with the most famous (horrific) example being Rosemary Kennedy, whose politically famous family lobotomized her in part because her antics publicly embarrassed them. She never recovered from her lobotomy, and spent most of the rest of her life in an institution.
X. TERRITORIAL DISPUTES
I used to be confused about something extremely basic. Why are there so many professions dedicated to the brain? There are psychologists, cognitive scientists, neuroscientists, psychiatrists, neurologists, and neurosurgeons, among others. And these are all obviously different, but also somehow kind of the same.
This is partly due to a difference in commitments. For example, a cognitive scientist is interested in understanding not every aspect of the brain, but most particularly the aspects important for cognition and intelligence. They acknowledge that the brain is composed of biological ‘stuff’, like neurons, but think it may be more fruitful to view the brain more abstractly as performing computations in order to solve survival-relevant problems. A molecular neuroscientist, meanwhile, is intensely interested in the specifics of the molecular biology of neurons, and tends to think that this low-level biology will tell us something important about how the brain works. It’s like the standard joke about the elephant: we’re all blind men touching different parts of the same thing.
But I don’t think the difference in commitments is the full story. The many professions are also in part due to what one might call territorial disputes that play out over decades. Why does the ‘psychiatric nurse practitioner’, who in many places can do most of the things an MD psychiatrist can do, exist? Because there are groups of people fighting each other for patients and legitimacy!
Valenstein thinks that a few territorial disputes explain some of the dynamics of the history of psychosurgery. The most important is the clash between those who subscribe to a functional theory of mental illness, which suggests it is primarily due to life experience, and the organicists who think it is mostly due to biological factors. In addition to each group having different beliefs, they also both wanted professional clout and access to patients. But if you believe your rivals have a totally wrongheaded view of mental illness, why should they get recognition? Why should they be the first line of attack? Conflict is inevitable.
He traces some of this history in the very first chapter of the book. Early in the twentieth century, there was a heated battle between the neurologists, who mostly took an organic view of illness, and the psychiatrists, who after Freud largely subscribed to a functional view. The neurologists were losing this battle for patients and prestige when psychosurgery began in 1935, and the victory was essentially complete by the end of World War II. Some of the details of the dispute are funny: for example, when a joint certification board was established, some were angry that “Psychiatry” preceded “Neurology” in its name, “in spite of the argument that n precedes p in the alphabet.” (ch. 1, p. 22) Neurologists were also squeezed out of their turf by neurosurgeons, since they had to refer patients to them to do the ‘real’ work, e.g., operating to remove brain tumors. Some pejoratively called them the “pimps of neurosurgeons”. (ch. 1, p. 17)
But then the psychiatrists became threatened by the unwashed (or at least, not medically trained) hordes of psychologists, who could also do talk therapy. It was to the disadvantage of the psychiatrists that the popular Freudian methods did not really require much training to do, even if they could argue substantial training was required to do them well. This led psychiatrists to try to distinguish themselves from the psychologists, and one of the ways this happened was by embracing somatic therapies: therapies which involved physically manipulating the body, like insulin coma and electroshock therapy. Clearly their use was a sign that psychiatry was ‘real medicine’, and not just talk therapy plus metaphysics. Ironically, this professional attack from psychologists pushed many psychiatrists closer to an organic view of mental illness, since the ‘success’ of the somatic therapies was thought to have a biological explanation. For example, spinning patients around in a whirling chair was thought to improve brain circulation, and hence (hopefully) do something to combat mental illness.
This embrace of somatic therapies is in part what made psychosurgery popular. It was understood that talk therapy, which could require many sessions over weeks or months, did not scale to the setting of the overcrowded state hospitals. And furthermore, it wasn’t thought to be effective on many of those patients. Psychosurgery was ‘real’ medicine, and seemed to work.
Another relevant dispute is the one between the somatic-therapy-embracing psychiatrists and the neurosurgeons. Once he began advocating for the transorbital lobotomy, Walter Freeman suggested that psychiatrists in state hospitals across the country should be trained to perform lobotomies. Moreover, he thought they did not need the help of neurosurgeons, who were too expensive and generally required resources these hospitals did not have.
Predictably, neurosurgeons both viewed this as unsafe (see earlier comments about a lack of gloves and anesthesia) and as an encroachment upon their turf. Valenstein argues that the vocal resistance of many neurosurgeons to the transorbital lobotomy contributed to more widespread concerns that all lobotomies were dangerous and should not be used—which is ironic considering that neurosurgeons usually only had a problem with the transorbital variant performed by psychiatrists. An internal dispute grew out of control and threw a shroud of disrepute over the whole business.
XI. ECONOMICS
This reason Valenstein gives for the prevalence of psychosurgery might be the easiest to understand of all. Yes, people wanted to cure the sick. But realistically, it was unlikely that most severely mentally ill patients would significantly improve. If they could not be cured, perhaps they could be made more agreeable—and hence easier and cheaper to care for.
State hospitals were horrendously overcrowded. If lobotomy truly treated patients, they could be sent home (which reduces costs). If it didn’t treat them, but merely incapacitated them, that was still a net benefit from the hospital’s point of view: formerly violent patients would no longer need to be restrained (which reduces costs). If it killed them, that would be cheaper still.
In 1941, the superintendent of Delaware State Hospital spoke out in favor of psychosurgery during a panel discussion at an American Medical Association meeting. He lays out this logic in a fairly straightforward, if cold, fashion: (ch. 8, p. 154)
From an economic point of view I should like to give some figures as to what this may mean to the public. We have come to the following conclusion with regards to our own cases: In our hospital there are 1,250 cases and of these about 180 would be suitable for such an operation. In our hospital these patients could be operated on for $250 per case. That will constitute a sum of $45,000 for 180 patients. Of these we will consider that 10 percent, or 18, will die, and a minimum of 50 percent of the remaining, or 81 patients, will become well enough to go home or to be discharged. The remaining 81 will be much better and more easily cared for in the hospital. Thus the hospital will be relieved of the care of 99 patients. That will mean a saving of $351,000 in a period of ten years. I believe that, these figures being for the small state of Delaware, you can visualize what this could mean in larger states and in the country as a whole.
Valenstein adds: (ch. 8, p. 154)
This economic argument was frequently raised throughout the period of expansion of lobotomy. In 1948, John Fulton remarked that if only 10 percent of the patients occupying neuropsychiatric beds could be sent home, “it would mean a savings to the American taxpayer of nearly a million dollars a day.”
Interestingly, this dimension of Valenstein’s argument also explains psychosurgery’s decline. It arguably did not decline for moral reasons, since the obvious objections had been raised and debated for well over a decade; instead, it declined because it was outcompeted. Psychoactive drugs were cheaper, safer, and required much less training than brain surgery. The timing of psychosurgery’s decline precisely coincides with their introduction.
XII. DO NO HARM
By now, you’ve probably figured out what I’m going to say. It’s been forty years since Great and Desperate Cures was published—and in some ways, not much has changed. The state of affairs in 1986 remains so apt today that I can’t help but liberally quote from Valenstein’s assessment: (ch. 16, pp. 291-292)
It is indeed all too easy to look back on the past and wonder complacently how prefrontal lobotomy could have been so readily accepted. Oblivious to the similarities between past events and present practices, we draw no lessons—as though, for a brief period, psychiatry, responding to unique circumstances and the influence of a few zealous, if not malevolent, physicians, had run amuck.
Although it may be comforting to believe that the forces responsible for the wide acceptance of prefrontal lobotomy and the other somatic therapies described in this book are all behind us, they are, in truth, part of the very bone and marrow of the practice not only of psychiatry but of all medicine. There are today no fewer desperate patients and desperate families; premature reports of spectacular cures with minimal risks are still accepted uncritically; the popular media promote innovative therapies even more enthusiastically; economics is no less an influence on the selection of treatment; conflicts persist within and between specialties; and ambitious physicians still strive for “fame and name.”
There is such a (deserved) stigma surrounding psychosurgery that I doubt something like the lobotomy will be popular any time soon. But the mistakes of the past are not usually the mistakes of the future; history rhymes rather than repeats. The forces Valenstein mentioned may not have conspired to produce a new rash of lobotomies, but have produced (i) the rise and fall of Theranos, (ii) the opioid epidemic, and (iii) academic fraud surrounding the amyloid plaque explanation of Alzheimer’s Disease, among other issues. And these are just some of the more popular scandals known to laymen.
What should we do? In an ideal world, we might only attempt treatments whose effect on patients we understand. After all, the human body and brain are extraordinarily complicated, which yields tremendous uncertainty regarding any intervention on them; it seems unfair to put patients at risk when we are so uncertain of what might happen.
But we probably can’t do this. As Valenstein observes (ch. 16, p. 295), we lack an adequate mechanistic understanding of most treatments, and requiring physicians to only use treatments we understand would leave them with no tools:
If we were to reject treatments whose effects we did not understand, even aspirin would not have been acceptable during most of the period of its use. Despite the enormous amount of research on the biochemical action of psychoactive drugs, there is no agreed-upon explanation of how different drugs help anxious, depressed, manic, obsessed, and schizophrenic patients. Psychoactive drugs are used extensively because they are effective and convenient, not because of any compelling scientific rationale. Indeed, the first psychoactive drugs were discovered accidentally, and only afterward were theories developed of how they might work. Similarly, electroconvulsive treatment is considered by approximately 70 percent of psychiatrists to be effective in alleviating otherwise intractable depression, despite the rejection of the original rationale justifying its use and no agreed-upon explanation today of how it works. In medicine, we have to be most influenced by the quality of the empirical evidence that a treatment does more good than harm.
This world is far from ideal, and we must be content with trying things we do not understand theoretically, but which have some record of empirical success. Valenstein continues (ch. 16, p. 295):
Where no effective therapy exists for desperately ill patients, equally ethical and knowledgeable physicians may disagree about treatment. Some risks have to be taken, and some harm will inevitably ensue along with some benefit.
If we’re stuck with experimenting, what do we do? While Valenstein admits harms are inevitable, he does not think large-scale scourges like the lobotomy are. He suggests that ethics safeguards are essential; harm can be limited, for example, if dangerous experimental surgeries are at least not widely attempted before their consequences are better understood.
As a model of what he’s looking for, he points to something which at the time was relatively new: the requirement that novel drugs are approved by the Food and Drug Administration (FDA) in a process that generally requires both animal testing and randomized clinical trials. Although much has been written about how onerous these processes have become, I think most people would agree that it is good that they exist in some form; the modern debate concerns how thorough these vetting processes ought to be, not whether they should exist at all.
Valenstein suggests that a similar approval procedure should be required for novel surgeries. In 1986, no such approval process existed—and in 2026, it still doesn’t exist! I’m not completely sure why, but a 2017 article I found in the Cornell Journal of Law and Public Policy suggests it has to do with, among other things, fundamental differences between drugs and surgery. It is harder to run clinical trials with high statistical power for new surgeries than for new drugs, and it somehow seems more dubious to do ‘sham’ (i.e., fake) surgeries on real patients in order to have adequate controls. There is also substantial variation: while a drug is the same everywhere, the teacher-student way surgical knowledge is spread means that there are great differences in the details of surgery from place to place.
On the other hand, this does not mean that there are no safeguards. In the decades since 1986, hospitals have erected additional barriers to testing novel surgeries on patients, including the much-beloved institutional review boards and approval procedures for using new tools in surgery. And, of course, enough discussion of ethics concerns and lawsuits to freak people out, which creates a culture of wanting to avoid risks, at least to one’s pocketbook.
Is there any modern day analogue of the lobotomy? If there is, it can’t be completely obvious, since otherwise no one would do it. I don’t think there’s anything that could be fairly called a modern analogue. But there are still risky treatments done today which are known to be potentially harmful and which still lack any satisfying theoretical justification. Electroconvulsive therapy (ECT) is still done, albeit not at the voltage levels and frequencies that used to be typical, as far as I know.
In the 1960s, it was still used as a punishment in insane asylums. When Howard Dully was in one as a teenager, he recalls (My Lobotomy, ch. 11, pp. 173-174):
Throughout all of this, I had one really good reason not to get in trouble. There was a doctor at Agnews who believed in using electroshock therapy as punishment. Everyone knew about it. I think the technicians wanted us to know about it. They wanted us to know what was in store for us if we got out of line.
Steve was one of the people who got out of line. He was friendly with me, but with other people he could be real belligerent. He was a fighter. One day they took Steve out and kept him for a while. A week later, I heard he was out—but they’d moved him to a new ward. They had given him the electroshock.
When I saw him again, he wasn’t right. I don’t think he was ever right after that. The treatment was supposed to “calm” patients down. In Steve’s case, the calm was only temporary. Years later, Steve would be sent to jail for shooting a wino in the eye with a BB gun after the wino had passed him a bottle of wine that someone had urinated in.
In Great and Desperate Cures, Valenstein notes that this liberal use of ECT may have been problematic (ch. 12, p. 246):
Today, we might wonder whether some of her limitations were not the result of fourteen years of confinement in a mental institution where more electroconvulsive shock was surely administered than would now be considered safe. It is generally accepted that massive doses of electroshock are likely to produce memory and other cognitive deficits.
Anecdotally, although ECT has gotten much safer (due to the aforementioned reduction in typical doses and frequencies of treatment), a physician told me that they saw a problematic pattern at the ECT center of a major university: the treatments were not very tailored. They would do one patient every few minutes, and not change the voltage dose for different patients. This is probably partly because they may not have had good evidence that tailoring the dose changed things much. But it still seems strange to me.
In any case, years of research has also shown that ECT can help patients with treatment-resistant catatonia and depression. It has a track record of helping people when other tools have failed. My point is not to cast aspersions about ECT specifically. My point is just to argue that, when we coarsely intervene on the brain—whether as in ECT, the lobotomy, or other procedures—we ought to be extremely careful! And this is especially true when there is no agreed-upon theoretical basis for our interventions, which is still a problem with ECT in 2026.
XIII. THE MASTER OF EVIL
How invasive brain surgery impacts cognition is an interesting question for neuroscientists, psychologists, and cognitive scientists. Why psychosurgery persisted in spite of its obvious harms is an interesting question for sociologists and historians. And whether it was ultimately right or wrong is an interesting question for philosophers. For example, would a utilitarian approve of the lobotomy? What must their utility function look like in order for them to approve?
But we ought to remember that this dark and shameful history is not abstract. Real people suffered as a result of the decision to perform psychosurgery. Let us now return to the case of Howard Dully, who I mentioned in passing in the introduction. Freeman lobotomized him when he was twelve years old. (Freeman also operated on a number of slightly older children, which did not help his public relations efforts.)
Dully’s memoir, My Lobotomy, tells his story. It is one of the most heart-wrenching, depressing stories I have ever read. Dully’s mother died during childbirth when he was six years old. His father, Ronald Dully, went on to marry a woman that hated Howard. Not only was she a poor stand-in for his mother, denying him basic affection and support, but she mentally and physically abused him for years. Any child would have had a difficult time adjusting to that sort of treatment.
And then they made him get a lobotomy!
Decades later, Dully found the notes Freeman took on his case in an archive on Freeman’s life and work at George Washington University. Fortunately for Dully (and us), Freeman had a habit of taking detailed notes on all of his patients. The details of the encounters that ultimately led to the lobotomy are infuriating.
Dully’s stepmother went shopping for psychiatrists. She went through six, each of whom told her Howard was normal, before finding Dr. Freeman. Worse, his stepmother was not content to simply tell the truth regarding Howard’s behavioral problems; she had to invent some. She claimed he was violent, disgusting, and even that he hoarded feces (My Lobotomy, ch. 6, p. 78):
He still sometimes defecates in his pants or in bed or on the floor, or may wrap up a turd and hide it in the drawer; recently he urinated on the wall of his room; at another time he dribbled from his room all the way to the bathroom; used toilet paper can be found in his closet or in his bed or in the tub.
Dully adds (p. 79):
Those were the notes from Lou’s [his stepmother] first visit. Could any of it be true? I’m sure I didn’t wash well enough to satisfy Lou. I might have stained my underpants, or dribbled on my way to the toilet. I’m sure I blew my nose and dropped the tissue on the floor. But, wrapping up a turd and hiding it? Come on!
In her worst fabrication, she claimed that when Howard was five years-old, he was angry at the baby his mother had shortly before she died—and violently attacked that baby in its crib.
Freeman, despite probably not having the standing to do so, diagnosed Howard with schizophrenia, and made plans to operate on him swiftly. His father, probably pulled in a million directions by his multiple jobs, did not agree with his stepmother’s assessment but figured she and the doctor knew best. He gave his approval. He was lobotomized.
If the incident would have ended there, it would have been a terrible, horrific tragedy. But his stepmother still hated him. She probably expected him to become a nice kid, or a vegetable, or something other than a more scatterbrained version of himself. After he recovered, she could not stand his continuing to be in the house, even if he did not actually cause trouble.
The misfortune continued. He went to a foster home, and adjusted well, but was removed from it by his parents (probably out of pride). He went to a juvenile detention facility for a year. He went to an insane asylum for a year—not because he was insane, but because his parents had nowhere else to put him. He went to jail. He was homeless. His family, except for his father, essentially cut contact with him. He didn’t see his brothers or stepmother for years.
Howard recounts episode after episode in which he demonstrates poor judgment in the life that followed his lobotomy. He does petty crimes; he chooses bad romantic partners; he freely cheats on those partners; he is loose with the little money he does have, most of which comes from regular government checks. In many cases, Howard says that he acted out because he was “bored”. The memoir never explicitly says this, but given that extensive frontal lobe damage is associated with poor decision-making and executive control—consider the well-known case of Phineas Gage using more vulgar language, gambling, and being unable to hold down a job after a tamping rod destroyed a large chunk of his frontal lobes—it is likely that at least some of these issues can be attributed to the lobotomy. Being abandoned by your family and being thrown into the world with little preparation is difficult; enduring this after a lobotomy sounds impossible.
Not everyone liked the memoir. Some Goodreads reviewers think lobotomy victims ought to take more personal responsibility.
The arc of the memoir is to claim that, despite everything he had gone through, Howard came out the other side okay. He had kids; he had a wife that loved him; he finally got a job he enjoyed; and he found peace. In some ways these things are true, but Howard’s life was far from normal, and was disastrous in almost every sense one could imagine. His kids were unplanned, his good second marriage followed a terrible first marriage, and his bus driving job is not the one he was hoping for; he went to school later in life hoping to get a computer-related job. Even after NPR covered his story, he continued to have financial problems and health challenges.
Despite his presumably noble intentions, I think it’s fair to say that Freeman literally ruined Howard’s life. Similar consequences follow other interventions gone wrong. Whenever we reflect on the power and promise of science and medicine, this simple fact is worth keeping in mind.
For what it’s worth, I think Freeman was genuinely concerned for the wellbeing of his patients. Even Valenstein doesn’t think he was a monster. Here’s an excerpt from a 2005 NPR interview that included him:
CONAN: Dr. Freeman, it's also important to remember, was one of the top men in his field, at the peak of his profession, in 1949, when this operation was first developed, and yet he's remembered today, Dr. Valenstein, as, I guess, maybe second to Josef Mengele, as a monster. Is that deserved, do you think?
Dr. VALENSTEIN: No, I don't think that's deserved. One has to consider the times. We already talked about the fact that there were no other treatments available. Lobotomy in America was not all Walter Freeman. This was part of mainstream medicine. The most prestigious medical schools practiced lobotomy. Columbia University engaged in a huge project called the Columbia-Greystone Project. Greystone was a state hospital in New Jersey, and Columbia University staff were studying and performing lobotomies. So it was widely accepted, not only as evidence the fact that a Nobel Prize was given, but people talked about, even in prestigious medical journals, like the New England Journal of Medicine—they described lobotomy as ‘ushering in a new era of scientific psychiatry.’
He was fastidious about checking in with his patients, even decades after he had given them lobotomies. He had a box full of Christmas cards he received from his patients. (To be fair, he was the one that initiated correspondence.) Even if he was blinded by his ambitions, he still did care.
In 1933, the same year he finished a book on neuropathology, and a few years before he learned about and pursued psychosurgery, Freeman wrote a thirteen-stanza poem that Valenstein calls “prophetic”. It depicts the “Master of Evil” and his sons “Hurry”, “Flurry”, and “Worry” pushing Man to his “breaking point”—not through physical torture, but by assaulting his mind. It ends like this (ch. 7, p. 138):
… Then said Worry unto him: “All this of
which my brothers have spoken can I do,
And more also in addition.
For I can work upon Man’s imagination,
That same power with which he develops his
theories and his machines.
I can cause him to foresee events, both those that
will happen and those that will not.
I can cause him to interpret falsely the actions
of his friends
And of his family
And of the wife of his bosom.
I can cause him to fear decisions.
And to brood over mischances.
And I can cause him to lose sleep in prospect
of the morrow.”
“Tis best of all,” said the Master of
Evil, “For sleep would defeat our
every object.“Go ye three upon the Earth
And burn the candle of Man’s life at
both ends.
Spare not his frontal lobes where intelligence
And ambition
And judgment
And self-control
Are centered …”
Your message is stored now and emailed to the author after the contest ends. The author can reply to you, but their identity stays hidden unless they choose to respond.