Human: Solving the Global Workforce Crisis in Healthcare
March 2023
Introduction
In the eighteenth century, much of the metal objects a household owned – cutlery, crockery, horseshoes, carriage parts, weapons and tools – were produced by expert, professional blacksmiths. They dedicated their lives to the profession and honed their skills with a lifetime of expertise. As a result, they were a respected profession in historical societies – they form part of the pantheon in many classical religions. A single blacksmith would be trained to produce a huge range of items: the production techniques of the day and the scale of demand meant it was most effective to have a craftsman with the skills to produce whatever was needed. Over time, however, industrialisation challenged that model and blacksmiths now scarcely exist as a profession. Today, such objects are mass-produced separately in factories that specialise in the production of a single item. Generalist training, across a range of blacksmithing skills, has been replaced by an economy that hones the productivity of one particular product. As a result, access to materials and products that would otherwise have cost far more and been much scarcer, has been increased for billions of people worldwide. Healthcare must now embrace that same shift – if health services of the future are to meet the demands placed on them, they must move away from a profession-based model, towards one of functions, capabilities and industrialisation.
Figure 1 Human: Solving the Global Workforce Crisis in Healthcare
As populations grow, age, and survive illness (rather than succumbing to the short fatal battles of the mid-twentieth century) demand for increasingly complex healthcare services will grow. Increasing rates of multi-morbidity and poly-pharmacy will require clinical staff to be expert generalists, balancing a growing ledger of symptoms and interventions. At the same time, the frontier of knowledge will be pushed out, and increasingly advanced technologies will require greater levels of specialism amongst the medical workforce. With these increasingly sophisticated treatments, the expectations of the public will rise, both in terms of the level of personalisation, the efficacy of treatment and the quality of service from healthcare providers. Healthcare will need to be industrialised, personalised, generalised and specialised all at the same time.
Human: Solving the Global Workforce Crisis in Healthcare (henceforth referred to as Human) correctly calls out the challenge faced by healthcare workforce shortages. It describes a comprehensive list of the immediate and short-term actions for addressing this gap. Though Britnell’s background is in the British NHS, he reflects on challenges and solutions from across the developed and developing world: from Brazil to the United States, via China, India, and the Netherlands (among others) along the way. These solutions should be enacted, with minimal delay, to prevent the immediate scarcity of healthcare workforce resulting in rationing of care or falling standards.
By squeezing every drop out of the solutions put forward, Britnell estimates the measures in Human might increase capacity by 20%. While this is massive untapped capacity in the short-term, it pales in comparison to the long-run challenge: Between 1990 and 2017, the global burden of disability increased by c.50%. The rate will only increase as populations live longer, unhealthier lives. Healthcare systems, politicians, policy-makers and patients need to engage with more radical transformations, including reappraising some of the traditional pillars of healthcare, if they are to hope to tackle the problem in the long-term. That more radical reform means uncoupling clinical knowledge from clinical professions, as massively scaling the number of patients that a single clinician can effectively provide care for.
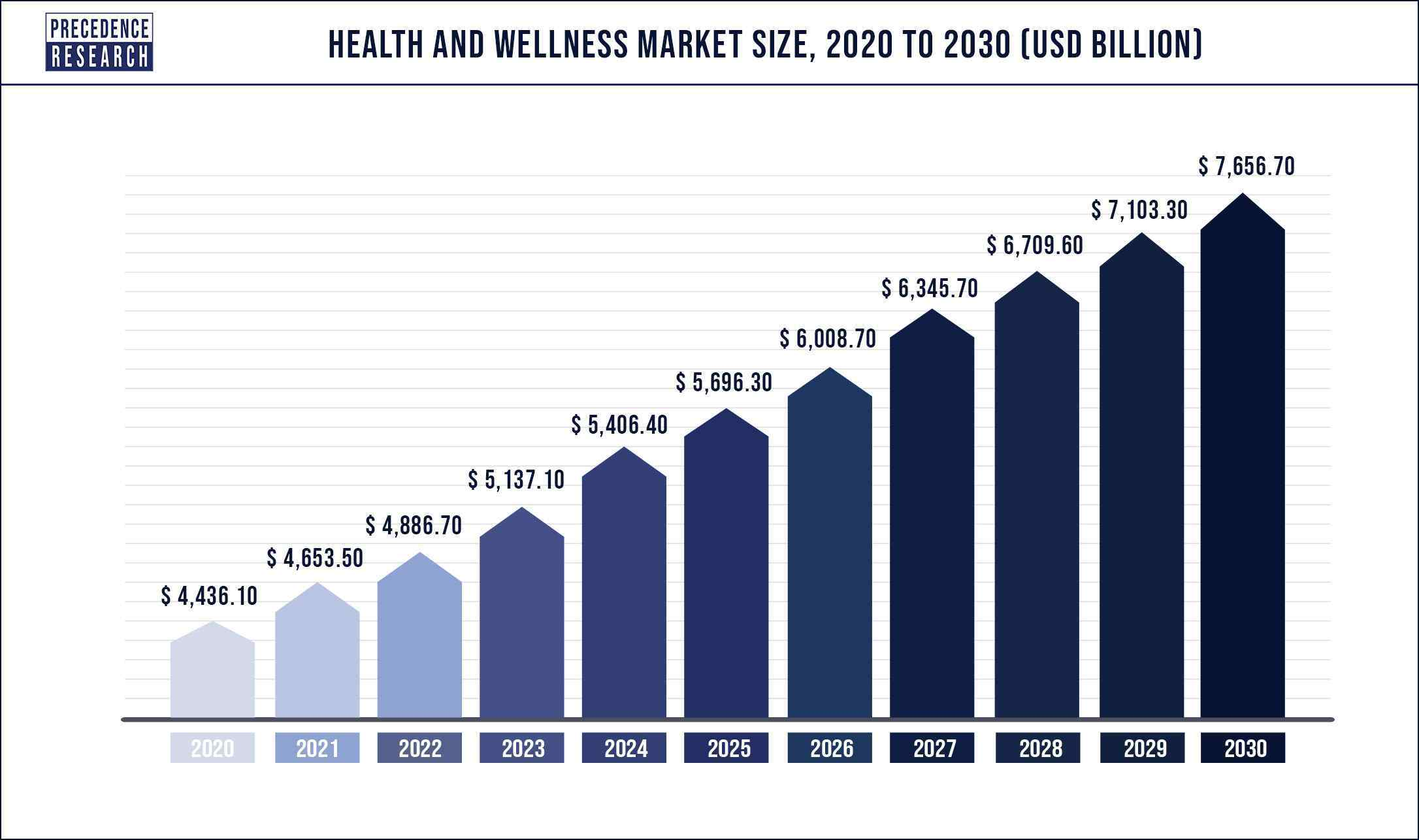
Figure 2 Healthcare expenditure (and demand) will continue to skyrocket, outstripping supply
The present paradigm of healthcare delivery – the model of supply that is supposed to meet this rising demand – is one of a ‘People Industry’. Currently, at the centre of any healthcare system in the world is a doctor, nurse or allied health professional who will prevent, diagnose, or treat your ailment. Accessing healthcare services means accessing one or more of these professions. This is for good reason: for centuries, the knowledge that underpinned effective health and care was complex and far-reaching. Without years of training, access to specialised learning material and a space to develop medical skills, ordinary people could never hope to equip themselves with the know-how to correctly diagnose – let alone treat – their diseases.
The 21st Century, however, offers a new way of supplying healthcare services: converting health and care from a ‘People Industry’ to a ‘Knowledge Industry’. Instead of navigating patients through complex systems to the correct professional, technology should allow modern health systems to instead direct patients to the correct information (the right diagnosis, the right medication, the right dose) to treat their ailments. Doing so will require decoupling ‘People’ and ‘Knowledge’ and, in doing so, a radical transformation of existing healthcare professions. Like the blacksmiths of old, current healthcare professions will be removed (or radically reframed) by new ways of delivering healthcare that allow patients to engage on an industrial scale.
What is the scarcity in the healthcare workforce?
Britnell is a true healthcare expert: during his career, he has been the Chief Executive of one of the largest UK hospitals, a senior mandarin in the Department of Health, and chairman of KPMG’s healthcare, government and infrastructure function. In the latter role, he advised healthcare providers and governments in more than 80 countries. It is therefore to be expected that his diagnosis of the biggest problem facing healthcare is precise, detailed and evidence-based. Governments and healthcare providers are facing a torrent of challenges in the next decade and beyond – financial pressures, capacity constraints, rising public expectations, pandemic recovery, an unmanageably broad range of technological ‘solutions’ (some more valuable than others). Calling out workforce shortages in healthcare is not new, but providing exclusive focus on it as the most important issue is valuable. Britnell pinpoints the capacity, engagement and expertise of the workforce as the most important.
Britnell’s arguments about shortages are well-nuanced too, recognising not only the global shortfall, but also the uneven distribution. This includes uneven distribution between different clinical specialties or geographic regions. Scarcity is exacerbated in the developing world and rural areas of the developed world by ‘care deserts’, with trained professionals following the opportunity to urban areas in the developed world. He describes the ethical dilemmas of international recruitment, and particularly the importing of skilled professionals from the developing world to the developed world. While this can provide opportunity for the individuals who migrate, fill material shortages in the destination countries, and supply training and remittances that can return to the nation of origin, it also deprives poor countries of much needed skills. Britnell describes the need for a thoughtful and planned approach to international recruitment.
Some commentators have suggested that investment in the healthcare workforce ‘pays for itself’ – the additional healthcare capacity results in greater productivity for the economy, which more than covers the investment needed. Britnell is sympathetic to this argument and suggests that government’s short-changing of investment in healthcare workforce has been false economy: restricting access to healthcare services costs more in the long-run. This is an attractive but unproven argument, allowing us to dodge the difficult choices between maintaining fiscal responsibility, investing in healthcare or cutting other public services.
Significant investment in healthcare does not necessarily translate to a more affluent nation or ‘pay for itself’. For example, UK healthcare expenditure rose by 64% from 2007 to 2019, while GDP fell by 7% over the same period. The number of doctors in the health service rose 41% in that time. Unlocking significant economic benefits from healthcare, to the point where it comes close to ‘paying for itself’ may be possible, but would require a laser-like focus on the aspects of healthcare that support the economy. For example, deliberate and explicit prioritisation of musculoskeletal and mental health services (the biggest drivers of long term sickness absence in the developed world).
Furthermore, there is also the risk of diminishing returns from the investment in additional healthcare staff. There is no correct upper limit to the amount of healthcare that a nation should deliver: as capacity increases, the bar for acceptable health (or the level at which healthcare services are needed) shifts. In the UK, whether consciously or subconsciously, primary care doctors (who refer patients for specialist help) hold back or send forth patients for hospital treatment depending on the size of the waiting list. As capacity increases, waiting lists shorten, and patients are referred with less serious needs, which might otherwise have been managed in a community setting. Over-supplying the healthcare workforce is not, therefore, risk free. For governments trying to manage healthcare expenditure, this begins to look like supply-induced demand: clinical activity that doesn’t generate outcomes that make it worthwhile. That is not to say that the current workforce supply is in the right place: there are clearly shortages (as Britnell describes) and areas of the world where patients receive unacceptable quality and experience of care.
We must confront the reality that the value in a high-quality healthcare service is not financial and it is unlikely to pay for itself. Health has value in itself, beyond economic returns: as a platform on which people can build meaningful, happy, independent lives with self-determination. Optimistic notions that ‘health is wealth’ and investment in healthcare will unlock economic productivity that mean we needn’t confront the financial trade-offs are for the birds. Over the long run, delivering high-quality healthcare, without significant limits on access, means looking for ways to lower the unit-cost of healthcare delivery. Otherwise, the investment needed to maintain a workforce supply commensurate with demand will either bankrupt a nation’s finances or leave other public services threadbare and impoverished.
Why does scarcity of healthcare workforce matter?
At its simplest, shortages of medical workforce results in restriction of access (patients, nearly always the poorest, cannot access services), reduction in quality (stretched staff spend less time with patients, or care is delivered by less qualified staff) or both. The US and UK health systems are broadly at opposite ends of the spectrum in the developed world: The US provides excellent care to a select sample of the population, while quality in the UK suffers as universal access is maintained. In either scenario, tackling the scarcity of workforce supply is crucial to improving healthcare outcomes for patients worldwide.
A scarcity of healthcare workers is currently the biggest bottleneck on quality and accessibility of healthcare. Physical assets – hospitals, scanners, operating theatres – are cheap and easy to produce compared to the time and money that goes to producing a single consultant (the UK equivalent of an attending physician). Estimates suggest that it costs around £250,000 ($350k) to train a doctor in the UK. Estimates rise to £1.1m for a doctor in the United States - about the same as a single brand new MRI machine (which will ‘see’ many more patients and not expect an annual salary or pension on top of the training costs). In the UK, it takes c.10 years for a newly-graduated doctor to become a consultant – a new hospital can be built in 4 years or less.
In the developing world, workforce scarcity is similarly important – though the problems may be greater or different, they still centre of the provision of a skilled, accessible workforce at scale. Britnell outlines the impact of the workforce shortage in India: only one in ten primary medical centres in rural India (serving a population of around 900m people) have a trained medical-trained doctor.
Up front, Britnell sets out some stark statistics on healthcare workforce supply: “By 2030, demand for health workers will rise to 80 million, but the World Health Organisation estimates there will be a worldwide shortage of around 18 million.” He suggests that workforce shortages are a critical driver of the huge gulf in life expectancy across the world: the average life expectancy of a citizen born in Sierra Leone is 34 years shorter than that of a person born in Japan.
Beyond a smattering of examples and perhaps because it goes without saying, Britnell is surprisingly quiet on the impact of workforce shortages on patient outcomes. The manifestation of understaffed medical services varies across the globe: in Brazil, it results in huge disparities (he cites, for example, an infant mortality rate in the north of Brazil that is double that of the better staffed south); in India, non-medically trained traditional healers step in to fill some of the void. In the US, healthcare workforce supply is one of the drivers of cost and is negatively impacting access to services. 97% of senior leaders in the UK cited workforce shortages as having “serious and detrimental impact on services”.
Britnell also reflects on why scarcity matters as a driver of further scarcity i.e. vicious cycle. As staff leave the profession and roles are left unfilled, the burden placed on staff that remain grows. In the UK, vacancies are routinely filled with long-term temporary staff - in some cases, the very staff who have left permanent employment in favour of better paying temporary positions. Administrative tasks (running the team, managing the rota, responding to complaints) fall to permanent staff and, as vacancies and temporary staff increase, the burden of this unsatisfying and bureaucratic work is increasingly placed on those who remain, increasing the likelihood they too will choose to leave.
Britnell outlines, in compelling detail, the moral and emotional toil that operating in an under-staffed environment places on staff. In the two scenarios described above – restriction of access or lowering of quality – staff are either asked to work in systems that do not provide the level of care staff would wish to provide, or staff work in systems, knowing that there are swathes of the population who cannot access healthcare services. Given the vocational calling associated with healthcare careers (for many, if not all, who work in them) and the desire to deliver real care for patients, these falling standards reduce morale further. In Radical Help, Hilary Cottam, describes the ‘burn out or numb out’ response of frontline public service staff working in over-stretched conditions. The Covid-19 pandemic, and the sub-standard levels of care that some staff were required to deliver or witness due to unprecedented demand on services, has further exacerbated this, leaving some staff with PTSD or burnout. Staff operating in under-staffed environments, where they feel unable to deliver the care they believe they should be delivering, are more likely to leave the service in desperation.
What are the drivers of scarcity?
Britnell lists a number of drivers of the global shortage. Top of the list is short-termist thinking by Governments, who have successively failed to grasp the nettle and increase training numbers. When confronted with the long-term consequences of under-investment, and the short-term need to demonstrate fiscal responsibility and balance competing political priorities, governments have demurred from long-term investment in the healthcare workforce. Given the long lead-times on training for healthcare professionals, why should a government, in power for four or five years, invest money now that will only bear fruit for their opposition? In particular, Britnell calls out nations where Governments set an artificial cap on the number of training places for doctors and nurses in a bid to control future spend and reduce supply-induced-demand.
Britnell identifies productivity – and keeping it raising at a rate commensurate with demand – as a key problem. He raises, but does not explore in detail, ‘Baumol’s Cost Disease’ – the rise in wages over time for workers that experience little or no increase in productivity. The archetypal example is that of musicians: the same number of musicians is needed to play a Beethoven string quartet today as was needed in the 19th century (the productivity has not increased), yet the real wages of musicians have increased substantially since the 19th century. In turn, as a “People Industry”, still based around the premise of getting a patient in front of the right professional, healthcare has also struggled with this phenomenon. It is not as straightforward as the musical example: productivity is notoriously difficult to measure in healthcare (since the outputs are hard to quantify or price) but academic measures show a general rise over time. The Office for National Statistics, in the UK, measures healthcare productivity as having risen 14% in the 25 years from 1996 to 2020. During the same period, the whole UK economy productivity growth was 26%.
However, the healthcare productivity rate rises to almost match the whole UK economy, at 24%, when quality-adjustment is carried out (although, as above, disability rose c.50% over a similar period). The productivity of healthcare, after all, doesn’t just measure the number of patients treated, but also the extent to which healthcare has improved their health. As more sophisticated medical therapies are developed, and treatments become more effective, healthcare productivity is recorded as rising, even if the same number of patients treated is the same. (If the modern quartet play Beethoven significantly better, has the productivity of the quartet risen?).
Ultimately though, healthcare is still based on a traditional ward or appointment-based system. The pattern of doctors’ ward rounds, operating theatre lists, outpatient clinics and face-to-face appointments would be as familiar to someone in the 1920s as it would be today. The sophistication of diagnostic equipment and operating theatres has developed, the range of treatments available has expanded, and (in some cases) the rollout of virtual technology allows appointments to be remote; but, it is still one doctor to one clinic, and one team of nurses to one ward.
Attempts to redesign the workforce, to increase the productivity of clinical staff through (e.g. new roles that can bridge professions, having less expensive staff take on more tasks, or expanding the staff empowered with particular rights, such as prescribing) have been hampered by unions and professional bodies. Unions representing doctors-in-training, for example, have suggested that Physicians Assistants[1] have taken on work that would have formed part of a doctors training (e.g. conducting routine echocardiograms). This is understandable but short-sighted: Professional bodies – such as Royal Colleges or medical societies – and unions exist to protect the interests of their members. Many of these reforms are about intended to increase outputs and lower costs, which often makes for less desirable work. Some of the reforms involve shifting tasks to cheaper or less qualified staff and reform is sometimes resisted on the grounds of worsening care or patient safety (though these are often unfounded and rarely weighed against a counter-factual of workforce shortages!). Substantial workforce reform to grow productivity will require taking on the vested interests of existing professions – handing privileges and status from a group of professionals to a wider workforce. It will also require, however, clinical leadership – the public will never trust workforce reform that has not come with the backing of doctors and nurses.
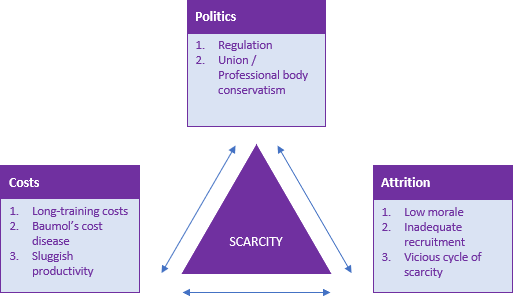
Figure 4 Each of the forces of scarcity feed of each other
Another key driver of scarcity, cited by Britnell, is professional regulation[2], specifically the “slow, expensive, adversarial and complex processes which act as a brake on innovative workforce practices (something readers of this blog will be familiar with). He points to, for example, the two and half (or more) years that it takes to amend professional regulations (and the laws they are based off). This creates a significant lag between the roll-out of technology and updated professional regulations. Furthermore, it makes it difficult to experiment with innovative, technology-backed workforce redesign. Transformative models cannot be tested without changes to regulation, but the regulations will not be changed unless there is pressing need and good evidence of the impact. He also explores how current education and training is largely delivered along professional lines, embedding silo working from the off, rather than encouraging healthcare professionals to operate as a multi-disciplinary team. The examples he cites are largely UK-based, though he suggests it is a problem across the developed world, with Canada being the frontrunner in moving to a less obstructive approach to professional regulation.
The third significant factor behind the scarcity of the healthcare workforce is a global issue with attrition and retention, largely driven by poor morale among the healthcare workforce. Britnell points to a 2016 survey of 17,000 doctors, with 54% reporting low morale. Human was published pre-pandemic, which is widely reported to have plunged healthcare worker morale even lower. He describes poor pay, high workload, and limited career progression as the drivers of low morale, and makes a number of valuable suggestions to address these issues (discussed further below). At the most extreme end, Britnell describes high rates of violence –even murders – towards healthcare staff, particularly in China.
Though Britnell doesn’t describe in detail, he touches on how the nature of clinical work and the demands of the job are also likely to have contributed to burnout and attrition. There has been little evidence-based discussion about how working conditions for healthcare staff has changed over the last century, beyond testy anecdotal assertions that either things are getting worse or that clinical work was tougher, “back in the day”. Changes to working patterns, like the European Working Time Directive, have reduced the number of hours that healthcare staff work, compared to the middle of the 20th century. On the other hand, workload has increased. In the 1950s, there was essentially no treatment for heart attacks (beyond ‘bed rest’) and the range of diagnostic tests available to a clinician was far shorter. Now, a typical hospital inpatient will receive a plethora of scans, blood tests, and protocolised management plans, all delivered by harried healthcare staff and often without recognition of the extra demands that innovation places on them.
An area Britnell doesn’t touch on, but which is likely to be relevant, is the medico-legal environment in which clinicians now find themselves working. There is also good reason to believe that a more litigious environment adds further pressure to healthcare staff. While treatment guidelines have become more complex and nuanced, the likelihood of deviations from guidelines occurring (and being recognised) has increased. The introduction of standardised treatment guidelines has been good for patients – it results in more reliable, evidence-based care - but it may well be harder for clinical staff.
It’s possible that all these workload and morale factors come together to create a problem of ‘expectations vs reality’. Many clinicians – doctors, nurses and therapists – decide to enter healthcare in their teenage years, while at school and picking degrees. Many will have their view of a clinical career formed only by TV dramatisations and perhaps a relative working in the field. Increasing workload, the shrinking of professional autonomy (as clinical guidelines become the norm), and the increasing threat of medico-legal or regulatory sanction rarely feature in the media. In the current system, some aspirants for medical school imagine high-flying careers as autonomous professionals, in the style of Hugh Laurie’s House, but find themselves delivering routine care, trapped by strict clinical protocols on one side and baying lawyers on the other. More radical reforms to the healthcare workforce, described below, may help to address this imbalance of expectation and reality.
What are the solutions described in Human?
Britnell puts forward a range of (mainly short-term) fixes for the workforce scarcity. His ‘Ten-Point Plan’ to address the immediate workforce shortages includes:
These can be broadly grouped into two categories: ‘increasing the number of staff’ and ‘using the staff we have better’. Growing the healthcare workforce seems like a no-brainer to fixing the demand-supply mismatch. In a number of developed nations, opposition political parties are making breezy claims about lifting training caps as if it were an obvious solution without difficult trade-offs. No doubt there will be need for greater capacity, to keep up with growing populations, ageing populations and rising complexity. But policy makers must confront the reality (as described above) that training swathes more doctors, nurses and allied health professionals comes with sizeable costs and is not a long-term solution. A portion of those who train to be healthcare staff (including your author) move out of clinical practice and the training investment does not pay off as additional healthcare capacity. All of this is pressure on the exchequer and is just perpetuating a race against an ageing population that cannot be won by training more and more people.
An entire chapter is dedicated to women in the clinical workforce and ensuring they are a) retained throughout their careers and (b) recruited in the first instance (he points to examples such as South Korea and Japan, with the lowest level of female participation in the healthcare workforce from OECD countries). Ensuring equal participation between genders (and across other under-represented groups) is a route to growing and maintaining the capacity of the workforce. There is still residual opportunity here for some, but not all, health systems.
Besides increasing recruitment, the other half of increasing the volume of the healthcare workforce is retention. Britnell has a thorough chapter on ensuring that trained healthcare staff are motivated, rewarded and incentivised to stay in the healthcare industry, addressing poor morale and the attrition driving scarcity. He cites international comparisons on levels of engagement and morale, as well as pay and recognition within society. This is undoubtedly an area that policymakers are rightly prioritising: an already-trained, experienced member of staff is clearly more valuable than a new recruit, and many health systems do not make it easy for staff to stay.
The list of interventions to increase the productivity of the workforce is thorough and implementing them will be key to ensuring that developed healthcare services can supply high quality care, without unjust or inequitable rationing or slacking of standards. Fundamentally, if the ratio between the number of patients that a healthcare worker can effectively and adequately treat is not increased, society will be fighting a losing battle to keep pace with demographic pressures.
Technology has long offered the promise of greater healthcare productivity, but it is often a double-edged sword. It allows new and better ways of delivering care, but can also be labour intensive or grow the demands on healthcare workers (allowing them to see and treat new cohorts of patients that would previously have gone without). For example, increasingly sophisticated electronic health records are a powerful tool for modern health systems. However, some of them rely on detailed and specific manual data entry by clinicians, which can actually increase the reporting burden placed on them. Having high-quality, standardised healthcare data, which can be shared and stored easily, is incredibly valuable, but that comes at a cost of clinicians’ time. Alternatively, technology innovations in virtual and remote care have made it easier for clinicians to care for patients in their own home, and monitor progress with increasingly more granular scrutiny, but this is expanding, not reducing, the clinical workload: hospital beds are rarely closed, when virtual wards are opened.
There has been good progress in the last twenty years, getting staff to operate ‘at the top of their licence’ (finding ways for professionals to take on increasingly more complex and technical tasks, freeing up more expensive staff to do even more complex work). Advanced Nurse Practitioners (a UK example) are experienced nurses trained to deliver technical procedures, from putting in central lines to conducting routine endoscopies. This allows for rewarding career progression for these staff and allows doctors to focus on non-routine cases. New roles have been created, such as Physicians Associates or Nursing Associates, to take routine tasks off doctors and nurses (respectively). As described above, progress here has been slowed, however, by professional territorialism and shroud-waving about patient safety.
Interestingly, new models of integrated care and greater activation[3] of communities and carers are the only two of Britnell’s solutions that touch on tackling rising demand. Both these measures are really about transferring demand to other, less constrained parts of the system or reducing low value activity. There is little about serious engagement with prevention, and tackling the rising tide of long-term conditions that will continue to submerge whatever workforce capacity we can create. Britnell appears to take the demand-side of the supply-demand mismatch out of the equation. This is a large omission – without addressing the growth in demand, healthcare systems cannot hope to continue to meet the supply requirements – but understandable, given the breadth and depth of this area (and the significant amount already written on it). While drugs like semaglutide may offer a deus-ex-machina solution, we cannot bank on fixing the myriad long-term conditions bearing down on society (dementia, diabetes, hypertension, depression, etc) before the burden has far outstripped the ability of health services to respond (with patients bearing the brunt).
There is surely value in both integration and activation, but difficult to unlock and hard to quantify. Integration[4] in healthcare is a broad term, which can mean different things to different people (even working in the same health system). The benefits are broad, but the evidence on what precisely unlocks value for patients and health systems is unclear. There are undoubtedly health systems internationally that are both integrated and appear to operate more efficiently and effectively (Britnell discusses Clalit in Israel, for example). But there are also examples where integration has been attempted but not realised the benefits promised. Supporters of integration dismiss these examples as having insufficiently or ineffectively delivered integrating transformations (“the data was joined up – sure - but teams never used it to change how they work_._”), while critics of integration cite these as examples as evidence of snake-oil. The reality is that there is not a clear description of ‘the best’ configuration of health services, or an effective roadmap for getting there. Integration may help us distribute demand, but is not a panacea and the evidence is still unclear on what really works.
Greater community, patient and carer activation is also nearly always a good thing – in part because the term activation can describe all the good things (better autonomy, better understanding of health and illness, greater cohesion, etc.), without reflecting on the bad. When done badly, families will be left to care for a sick loved one, without adequate support from healthcare services. Patients will be left to manage a condition they don’t understand, while healthcare services move on to treat the next patient. Those calling for greater activation of communities and patients often do not confront these downsides, but it is highly likely to be part of the reality. It’s also not clear that transferring caring tasks from healthcare workers to the members of the public (be they family or community) is more efficient for the economy as a whole. If the reality is someone having to leave their job to care for a family member, society would be probably be better off employing someone else.
All of these proposals have value, and taken together are likely to make a serious dent in the supply-demand mismatch. Some of them are not straightforward to deliver – changing a person’s relationship with family and what society expects in terms of caring obligation is not entirely in any government’s control – while some are merely a matter of additional investment and time. Fundamentally, however, none are a radical departure from the status quo model of healthcare delivery. Focussing only on training and retaining more doctors and nurses, is to become tied up in a perpetual arms race with demography. Ironically, given the title of the book, ensuring adequate (if not universal) access to high quality healthcare in the long-term will require a shift away from a model based on people.
What is the transformation that will be needed in the long-run?
The solutions outlined by Britnell will be critical to protecting health services in the near term (next 10 to 15 years), but beyond that, more radical reform is necessary. Britnell holds back from describing the more radical reforms below, perhaps from a desire to ensure his proposals appear reasonable and achievable, and are not rejected out of hand.
Healthcare has historically been considered – and is currently treated as – a people business. The systems and processes involved in modern healthcare are about connecting the right patient with the right healthcare professional. That may be a remote consultation with a family doctor or anaesthetised on an operating table, awaiting the surgeon. Even the myriad technological advances in healthcare of the last hundred years are either to support a clinical decision by a healthcare professional, or a more sophisticated intervention delivered by a healthcare professional.
Over time, this knowledge was refined and honed – the scientific method allowed determination of what was ‘correct’ medical knowledge and what was folklore or hokum. Professions – and professional accreditation – evolved to identify those individuals with access to the ‘right’ knowledge. The doctor replaced the village healer and midwives overtook doulas. Professional identity and regulation became a protection for patients, helping them access the right person – a proxy for the right knowledge.
In the 21st century, healthcare has the potential to transform fully to a knowledge business. It should be about connecting a patient with the knowledge about what ails them and what can be done about it. Pre-internet and digital connectivity, knowledge was stored and passed on in either physical books or the memories of people. It made sense to have a professional as the vessel for storing and imparting knowledge (and, importantly, identifying the correct knowledge and how to deploy it!). Doctors, through learning and experience, sifted huge reams of knowledge to identify a diagnosis and recommend a treatment. Lay persons would not have known where to start, trying to access the information in books, or by themselves.
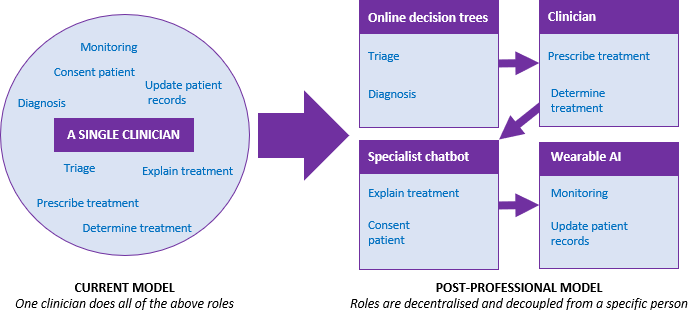
Figure 5 A post-professional model would see roles delivering individual tasks, supported by AI and technology
Some of this transformation is already underway. With the digital revolution of the 21st century, however, it has become increasingly easy for individuals to access increasingly complex and specialist knowledge themselves. Guided by search engines, apps, and algorithms, a person with little or no medical knowledge can be directed to an online form that can help them triage their condition. Verified websites (often designed for professionals) can help patients understand what the best treatment is for their conditions. Apps are now being used to support patients to manage their own musculoskeletal issues, to stop smoking or to deliver psychotherapy. Historically, all of these would have been delivered by a healthcare professional. Checklists and validated, evidence-based guidelines should be able to help people make sensible diagnoses, or at least triage conditions. Wearable devices are helping patients monitor their own conditions, in place of blood tests and investigations.
All of these advancements are positive, but are occurring ad hoc, rather than as a systematic transformation led by governments and healthcare leaders. Too many of digital resources are designed for use by clinicians, without the challenge of “what would it take for a patient to use this themselves?”. If healthcare services in the developed world are to survive the rise in expectations and demographic pressures of the 21st century, they will need to find away to uncouple the ratio of healthcare professionals to patients. The express policy priority for governments should be in finding technological solutions that remove the need for healthcare professionals as much as possible.
As healthcare becomes more diverse and complex, but information management systems, guidelines, clinical trials and standardisation become more sophisticated, we should consider the capabilities needed to deliver healthcare. The alternative – the system we use currently – trains a handful of professions, and asks them to deliver a wide range of clinical functions. Surgical ‘factories’ in India – described by Britnell – are a first step to this: consolidating all the procedures of one type into one place and delivering high-quality operations as efficiently as possible. The next question might be “do those doing the operation need to be doctors?” - Do they need to have been to medical school? Could an intelligent person with two years of focussed training remove a cataract, without learning about orthopaedic surgery, medicine, psychiatry, clinical communication or biochemistry? Does this person also need to be the one to see the patient recovering on the ward the next day – or could that be a different person, with different training and supported by guidelines and protocols to help them spot slow recovery or complications?
In medical specialties, too, a doctor will typically deliver a wide-range of clinical tasks, in different clinical settings, much of which is process or paperwork. For example, a typical day for a cardiologist might begin with a ward round: walking from patient to patient, asking a standard set of questions (perhaps nuanced, but within a framework), reviewing standard test results and recording the findings in the notes. How much of this could be proceduralised or automated, even if the relevant outputs are then reviewed by a cardiologist (potentially not on site)? Their afternoon might then be spent in clinic, seeing patients with heart failure. Again, how many of these patients could be met instead by someone taught how to conduct an effective patient interview, equipped with detailed background on heart failure specifically, and supported by clinical guidelines (and if necessary, a specialist doctor, as we would recognise them now, on the end of the phone)? This training could be delivered on the job, rather than in university, and would be much more focussed on the specific task, rather than current medical training which covers a bit of everything, most of which is then not used. The same cardiologist could instead deploy their expert knowledge on a much larger caseload, focussing on non-routine cases, providing ad hoc support to the above staff in difficult cases, or delivering research or education. Far fewer of them would be needed, for the same sized population.
AI and technology will be critical to this uncoupling of clinical knowledge and clinical professionals. Even without undertaking the notoriously difficult task of forecasting when we might have 'strong' AI that is as generally intelligent as a top clinician, there are obvious roles for 'weak' AI trained for specific circumscribed tasks and decoupling clinical knowledge and clinical professionals. The possible functions it might support include:
- Supported clinical decision making: The pool of medical academic literature is growing at a rate far higher than can be followed by a single person. Having AI sift, appraise and curate developments in medical science will help clinicians make decisions backed by the latest evidence (e.g. is this patient on the right list of medications for their condition, genetics and demography? A complex task for a human but a rapid calculation for a trained bot). Beyond decision making support for clinicians, AI will also be able to support patients to make decisions about their health, something which has not been possible until now. This should help patients make intelligent decisions about diagnosis and treatment, without needing to ask a physician.
- Automated diagnosis: As AI becomes better trained at engaging in dialogue with humans, a chatbot should easily be able to extract a clinical history and cross-reference that with literature and context, to reach a differential diagnosis, recommend investigations and initiate a treatment protocol.
- Communication, coordination and sign-posting: Chatbots will also be able to support patients in navigating complex healthcare systems. One of the most valuable functions of clinicians presently, is pointing patients to the next place they can find help (be that a formal referral to a specialist or a set of trusted resources online). It should also be easy for AI to provide the administrative functions that take up a great deal of clinical and non-clinical time (“when is my appointment?”, “can I eat grapefruit with this?”, “what are the results of my recent scan?”).
Humans will always be a part of healthcare – almost certainly for the duration of the 21st century, at least. Some interventions are physical tasks, which robotics are some-way from being able to deliver autonomously without any human supervision. Some tasks are too personal to be delivered without a human touch, such as delivering a difficult piece of news or eliciting the true concern behind a patient’s story. Some patients suffer digital illiteracy or exclusion and will need to be supported through the system. Some matters of judgement are so delicate that people are unlikely to entrust them to anyone but another human – whether we should give treatment a last-ditch attempt or make a loved one comfortable, for example. Expert clinicians will likely have a place (particularly in the early period) in training and directing AI, as well as helping navigate and lead ethical conversations about priorities. They will also be invaluable in building public support and trust in automated solutions. And for at least the next twenty years, Artificial Intelligence is unlikely to be able to wholly replace the experience and judgement of healthcare professional – weighing up a host factors, including social context, the individuality of a patient, ambiguous evidence, etc.
There are likely benefits from having a single individual with a wide breadth of medical knowledge and specific expertise in one area. They can spot problems and make a diagnosis in fields that are not their own, and in complex cases can balance risks and trade-offs between treatment plans for different conditions in one patient. However, these benefits are diminishing and the shortage of healthcare professionals will have a more significant detrimental effect on patients. As society moves towards hyper-specialisation, the level of input a specialist can provide in a field that is not their own diminishes. They will surely know more about other conditions than a lay person, but if they don’t have enough experience to manage the other ailments themselves, a second specialist is required all the same. A smaller number of these experts could manage a far greater number of patients if their time was optimised on tasks only they could deliver, and with the support of a much wider team. This will be a big change for many societies – if a patient is not in front of a doctor, they often feel short changed. Healthcare and political leaders should start a discourse with the public about the changing nature of healthcare – listening to their concerns and building a new system that patients trust. This should become the new norm and, if it speeds up access and improves experience, patients will likely accept it.
How might we get there?
Transitioning from the current system to a more capability-based system, built on jobs designed to fulfil a specific function, would require a move away from the handful of professions that deliver healthcare currently. Professions have served mankind well – they have often been characterised by skilled people with a vocational calling (often with an altruistic desire to do good for society), going above-and-beyond in the execution of their craft. As well as lengthy training, professionalism comes with a number of trappings that signify special or exclusive status. This might be a professional register or regulator, prefixes or postnominals, a uniform, social status or specific privileges (e.g. the right to prescribe). Professionals often accept difficult jobs or take personal responsibility for impossible decisions, out of a sense of duty from their profession.
However, professions, as they are currently formed, may be hindering society’s progress to this new system of healthcare delivery. With the exclusivity and status of a profession, comes territorialism and tribalism. The Ockenden review into maternity services in the UK found a reluctance from one professional group (typically midwives) to escalate care or concerns to other professions (typically obstetricians), for fear it was tantamount to admitting failure. These practices come about when one profession feel like the own responsibility for managing a patient, and that ownership becomes more important than identifying and delivering whatever the correct intervention is for the patient. As described above, representatives for professions have raised concerns about other groups of staff accessing training, perhaps out of a fear that it signifies a loss of exclusivity and therefore privilege for that profession.
Under a post-professional model of healthcare delivery, healthcare providers will be responsible for identifying who they want to fill roles and with who. This would be much more capability based – focussed on the ability for the candidate to fulfil the specific role – rather than broad professional vacancies (“this vacancy must be filled by a nurse” etc.). Regulators would shift from regulating individuals to regulating outcomes and providers – a move that has only become possible as electronic health records have allowed for detailed analysis of patient outcomes.
As well as lowering the barriers to entry to the healthcare workforce (something Britnell discusses too, though in a less radical form), this would make automation and technological innovation easier to implement. Instead of powerful professional bodies, regulators and unions resisting moves to automate tasks, providers would be able to focus on specific tasks and automate them, as has happened in a number of other industries.
It will also make it easier for key skills to transfer into the workforce. For example, clinical bio-informatics (e.g. using data science to investigate genetic links to specific cancers or treatments) could be filled by individuals moving from the sphere of data science into a bespoke roles in the clinical environment, without regulatory blockers requiring them to have had a medical degree or a professional licence. With the ability to create much more specific and bespoke roles, unshackled from traditional workforce professions, providers will find it much easier to transform and innovate clinical pathways.
Government and healthcare providers should support the development of the AI functionality described above, both in terms of research grants and creating a nurturing environment for commercial solutions. Government can also aid the development of accredited treatment pathways and protocols by creating definitive guidelines. Government-accredited guidelines, developed by chosen experts and regularly reviewed and updated, may help form part of the solution to the increasingly restrictive medico-legal environment. Guidelines, with clarity about what to do and when (including when to deviate or ‘ask for help’) can be used to empower non-professionals in clinical roles and protect them from fear of medico-legal repercussions.
As mentioned above, this transformation needs to be led by clinicians – a group of people with almost unparalleled trust from the public. Combining the burning platform of workforce reform with the mismatch of expectations and reality in a modern clinical profession may be a means of getting that leadership. It might be possible to describe different clinical roles more precisely, and match incentives to those jobs accurately. For example, a high-flying university student intent on a clinical academic career could focus on filling the role of the clinical case manager, overseeing a team that is caring for thousands and leading research and education in healthcare. Meanwhile, someone looking for a stable, respected job with a good salary (but who perhaps doesn’t have the academic platform described above) might fit nicely into a clinical delivery role – taking histories from patients in the ED, protected from an over-bearing medico-legal system by straightforward and validated clinical guidelines.
Conclusion
Human is an insightful and commendably broad discourse on the challenges facing healthcare services over coming decades. Britnell is right to call out workforce supply vs demand as the biggest challenge and his ‘Ten-point Plan’ captures examples of best practices from across the world. His solutions, however, will merely buy time – to face down the demographic pressures, rising complexity and increasing specialisation, society will need to re-think what it means to be a healthcare worker and what is really needed to deliver health services.
In the longer term, healthcare systems will need to look to radical workforce redesign if they are in with a chance of matching supply and demand. This means maximising the use of technology, taking tasks off skilled professionals wherever possible and supporting patients with technology to manage their own care. Existing professions will need to resist the temptation to hold on to existing privileges and should relinquish tasks to others. This will require governments and health systems to take a hard look at existing regulations and training. Industrialising healthcare will be a far-cry from the personal family doctor of old, but it will be the only way healthcare can keep pace with modern disease and prevent unmet clinical need that should not be acceptable in the 21st century.
Footnotes
- ↩
A new clinical role, recently regulated in the UK, which supports doctors in delivery of routine activities
- ↩
Regulation to ensure healthcare professionals are safe to practise and remain safe to practise throughout their career
- ↩
Supporting and encouraging communities, patients and carers to take on more caring responsibilities
- ↩
The join-up of workflows, data, funding, corporate functions, workforce etc. between home care, community care, primary care, hospital care and social care