Pregnancy: A British Husband’s Review
The First Trimester
I sat uncomfortably in a darkened room, next to my wife lying on a bed, staring at a monitor suspended above our heads. The screen lit up with mysterious black and white shapes as the sonographer turned on the ultrasound machine. It was time to find out how far along the pregnancy had come – and whether it was in a safe place, or dangerously stuck outside the womb.
It was only a couple of weeks since my wife had shown me a positive test. The first thing I wanted to know was the due date. This of course depends on how long she’s been pregnant, but the online calculators were giving impossibly long ages for the pregnancy so far – until I eventually twigged that pregnancy starts at two weeks. It was the first of many baffling things that year.
When a woman says she is eight weeks pregnant, that actually means the baby has been in existence for about six weeks. It’s counted from the woman’s previous cycle, so for the first two weeks of pregnancy, ovulation hasn’t happened yet and she isn’t pregnant at all: it’s impossible to be one week pregnant.
But even this isn’t quite right. Because most women’s cycles aren’t perfectly regular, once you start getting scans, the pregnancy is dated from an idealised notion of when the previous cycle should have been (but probably wasn’t). For a while, whenever I told people about the pregnancy, I complained about the dating method. But nobody else seems to find this surprising or confusing, except my dad. So I guess this runs in families, and one day my child will be surprised and confused too.
Having discovered the pregnancy, we naturally wanted a scan to look at the baby. In my wife’s home country of South Korea, mothers get an ultrasound almost every two weeks. But it turns out that in the UK, the National Health Service (NHS) will usually give you only two in total: one at week 12 and one at week 20. Is this enough?
It is possible in medicine to scan too much, even when the scan itself is non-invasive and almost riskless. For a perfect Bayesian, more information can only ever be good, but in reality we tend to overreact. Scans can lead doctors to treat something that wouldn’t have caused a problem, or to treat something that was unstoppable anyway. And they cause stress.[1]
So when your hospital refuses to test or treat an issue, there’s an important question: is this genuinely the best evidence-backed course of action? In which case you should listen to the doctor and do nothing. Or have they just prioritised resources somewhere else? In which case you might want to advocate harder for yourself, or go elsewhere.
In pregnancy, this question comes up a lot. To start with, I was concerned about ectopic pregnancy, where the fertilised egg implants itself outside the womb. From what I could tell from reading (not a doctor, nothing in this review is medical advice…), ectopic pregnancies cannot progress safely to birth, so they must be ended either naturally or medically, and can be quite serious for the mother. At 1 in 90 it’s a small risk, but not vanishingly small. As the first NHS scan is not until 12 weeks, the only way you’d know is if you get a stabbing pain and start bleeding (or other symptoms).[2] So that’s why we booked a private abdominal ultrasound, and were now waiting in the darkness to find out.
The sonographer was heavily pregnant herself. I wondered idly if she did her own scans, while she searched with the ultrasound probe. Suddenly the screen stabilised, and she pointed out a big black circle. “That’s the baby house, safely in the womb,” she said. The cursor moved to a white triangle. “And this is baby.”
We gazed at the tiny ball of cells, and peering closely there was even a little flicker of pixels that represented the heartbeat. Like many before me, my mind turned to Psalm 139: “For you created my inmost being, you knit me together in my mother’s womb.”
At this scan I also discovered that “baby” doesn’t take the definite article. It’s always just “baby”, not "the baby". I would say it’s because Baby is treated as a name, except that it also seems to be written with a lowercase b.
Whether or not you get a scan to look, the pregnancy usually becomes obvious when morning sickness kicks in. Morning sickness can be pretty grim and is very much not limited to the mornings, but on the plus side it tends to be a sign baby is growing well (although sadly not always). My main guide for the pregnancy was an economist’s favorite: Expecting Better by Emily Oster. If you want morning sickness medicine, Oster’s top drug recommendation is implicitly the doxylamine-pyridoxine combination.[3] But only one woman she spoke to took medication, as others were too nervous. In Korea this is marketed as Diclectin, and many women in my wife’s chat group were happily taking it.
In the UK the same drug is marketed as Xonvea. We asked our GP, but she said it was greyed out on her computer system which meant she wasn’t allowed to prescribe it. And as pharmacies need a prescription, that means it’s essentially unavailable – so I’m not sure why it’s marketed here and who gets to take it. We were offered Cyclizine instead, with the offputting words “if you really need it”.
First Trimester Rating: 2/5. Great character introduction, let down by confusing timelines and nausea subplots.
The Second Trimester
Pink and blue have a bad rep. When I was studying data visualisation, I nodded along to lengthy articles on how to show men and women on charts. These days you definitely can’t use pink and blue, they said, but that’s unfortunate because people intuitively understand pink and blue. So you have to use colours like pink and blue, but not pink and blue. Purple and green, or something.
More than once, I had a conversation where someone started telling me it’s useful to know whether baby is a boy or a girl so I can prepare the baby room. Then immediately realise what they’d said and bite it back. (Joke’s on them, I live in a one-bed flat, there is no baby room!)
So I was amused, and at first a little uncomfortable, to discover that Baby World is unapologetically pink and blue. Baby shops have big “It’s a girl!” and “It’s a boy!” displays in bright pink and blue pastels, with all sorts of pink and blue cake fillings, pink and blue confetti, and pink and blue balloons.
We went with the cake. It was blue.
 Colour scheme of a gender reveal party, according to Google Search
Colour scheme of a gender reveal party, according to Google Search
Then, I was led to believe, it’s time to start weight measurements and amniotic fluid scans. Oster seems to worry a lot about these being misinterpreted. Her midwife berates her for gaining too much weight (an experience shared by our friend in New York), even though it would be worse to not gain weight. And when, in a later pregnancy scan that’s known for being noisy, doctors appear to measure a low level of amniotic fluid in her friend, they whisk her away for sudden emergency induction.
But my wife’s midwives never even measured her weight gain, and told me they would scan for amniotic fluid only if baby wasn’t moving well[4] or the fundal length (belly size from top to bottom) was unusual. Again I had to wonder if this was the right approach, or just the hospital saving money.
After reading Oster’s book, I was, if anything, relieved that the NHS doesn’t measure amniotic fluid levels. However, I did wish they would measure cervical length. In Korea this is frequently and routinely measured throughout pregnancy: if it’s too short, women are advised to be careful, or to have a McDonald surgery (tie a suture around the cervix) to protect the pregnancy. In the UK it feels like we just hope the pregnancy takes care of itself: hospitals won’t measure cervical length unless the mother has a history of miscarriage. Is this because it’s the evidence-based best policy for the mother, or just the NHS conserving resources? Without data I haven’t seen, it’s impossible to say, but I’m leaning towards the latter. The stillbirth rate is 0.25% in the UK, 0.27% in the USA, but only 0.17% in Korea.[5] Proactive monitoring is surely part of the story.
It seems to me that the various monitoring and screening tests can be placed on a scale of their benefit for a typical pregnancy, a bit like this:
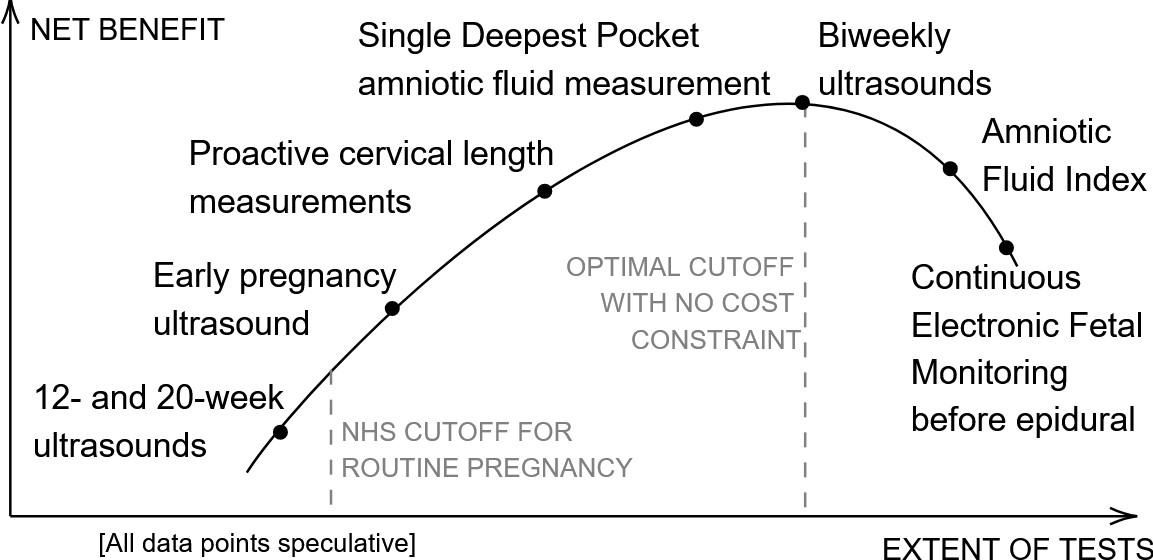
The basic ultrasounds are usually enough, then there are additional tests that make it slightly more likely the pregnancy will succeed and the mother will be safe. These get more and more marginal, until eventually some tests can apparently cause more harm than good,[6] because they lead doctors to overreact to noisy data. If you have the resources, you can try to buy extra tests to climb the curve until you are giving the mother and pregnancy the best chance you can.
Second Trimester Rating: 4/5. Strong set pieces, with compelling rising tension and ominous foreshadowing.
The Third Trimester
It was time to get ready for baby. Several friends and colleagues recommended we sign up for baby classes, which teach you about childbirth and baby care, so we dutifully enrolled. Only after enrolling did I hear the warning stories: one class where the men were told to sit against the wall so they would feel pain too, and one where a husband was asked to practise taking off a nappy, only to discover that the doll’s bottom had been smeared with peanut butter to make it “realistic”.
So I was slightly on my guard in the first class, and it wasn’t helped when we spent the first 20 minutes covering “what is a reliable information source”. After that however, the classes picked up. They covered information about local hospitals that wouldn’t be available in books, they were a good chance to meet other expectant parents, and if nothing else they were an interesting case study in pedagogy: how to keep a voluntary class of adults engaged.
 A C-section, according to our baby class
A C-section, according to our baby class
For the most part, the classes were balanced on the pros and cons of different birth and childcare options. However, the infant feeding teacher didn’t get the memo. She was a confident lady with a lanyard decorated with drawings of breasts, and a habit of answering a question with a question. “What if I don’t have enough milk?” one woman asked. “Do dogs worry about that?” replied the teacher. “Are you saying 100% of mothers can breastfeed successfully?” I followed up. “Would humans have survived if we couldn’t?” she answered.
She made it sound like the only possible reason for failure is lack of commitment. Don’t give formula, don’t buy bottles, don’t prepare a steriliser. This doesn’t chime with the stories I have heard from several mothers, and would have left us scrambling to buy supplies after birth, when the reality is that most families will do at least some mixed feeding. And it leads to the instruction not to give the newborn any formula, no matter how much they cry (advice echoed by Your Baby Week By Week); which in my opinion is pretty harsh, as some women’s milk supply genuinely isn’t enough to satisfy the baby until a few days in.
I do recommend baby classes, for a different reason. Childbirth and baby care are two of the areas where cultural differences loom the largest – not only between nationalities, but also between families and over generations. For example, Your Baby Week By Week expects you to go out with your baby in week 1, and Oster even talks about attending a party, while our Korean textbook advises not to leave the house or have visitors until at least week 7. If you and your partner have different information diets, you may end up with wildly different expectations without realising. So it’s useful to hear the same information and be prompted to talk everything through. But be careful: our baby class teacher once had a couple rage out of the room in a heated argument.
And the classes did prepare us for the 36-week hospital appointment, when the midwife asked for our birth plan. There aren’t many choices to make, but three of them are quite big: vaginal delivery v C-section, pain reduction methods, and home v birth center v labour ward. Depending on your answer to the first two, you might have no choice over the third: in the UK, C-section and epidural are labour ward only. (But you do get the choice, unlike in France: our friend in Paris wasn’t allowed an induction until week 42, or an elective C-section at all.)
Then we were posed a couple of questions in a very leading way.
- Skin-to-skin is great for baby’s health, and brain development, and breastfeeding, and mother’s recovery: do you want skin-to-skin? Yes/no.
- In the old days, we used to cut the cord immediately, but now we know delayed cord clamping gives baby a lot more blood and iron: do you want delayed cord clamping?
Actually I didn’t mind, because we were pushed in the right direction on both these questions. Delayed cord clamping carries a higher jaundice risk,[7] which neither the baby classes nor midwife mentioned, but I thought this was an acceptable trade-off for the blood and iron benefits. And skin-to-skin is widely accepted as a good idea, with no real downsides (one of the useful things the infant feeding teacher taught us, to be fair to her). We were told this needs at least an hour, soon after birth. Our friend in New York was told two hours. In Korea however, the baby is often taken away to a care unit, and barely sees the mum at all. If I were to sum up the healthcare systems, I would say that Korea is more mother-focused, while the UK is more baby-focused.
We weren’t asked about a doula. I was surprised because on the 80,000 hours podcast Oster said ‘get a doula’ is her number one piece of advice. Simkin’s The Birth Partner would agree. They make it sound like doulas are a very common and obvious choice. But what is a doula? Face to face, I never heard anyone suggest it.
A doula is a trained childbirth expert, who can accompany you to the birth and give support all the way through. I thought it sounded like a good idea – maybe because it would take responsibility off me as the birth partner – but we didn’t hire one in the end, partly because of the £1.5k price tag ($~2k). During birth, when I probably should have been concentrating on other things, I asked our birthing midwife how many people use a doula. In two years on the labour ward, she had seen only a single one, so they must be quite unusual.
To use the fashionable term, I did feel somewhat gaslit by the midwife appointments. More than once, I asked if it’s possible for baby to grow too big, only to be shrugged off with a blasé “oh no no no, that can never happen, the body knows what it’s doing” et cetera. Only when we got to the hospital for the big day, did they finally admit “yes there can be physiological incompatibilities…”. It was okay for us in the end, but our French friend’s baby didn’t have enough space and ended up needing physio. On the rare occasions our hospital measured baby, it was plotted on a graph and we were told how it stacked up in terms of percentiles. But shouldn’t this be measured relative to the characteristics of the mother rather than a generic distribution? Or actually measure the pelvic size to give a definitive answer like they do in other countries? Once again I felt there was room for improvement.
All of which brings us to the birth. The date of the birth is of course unknown in advance, although it’s possible to make a better estimate than the official due date. As with the start of pregnancy, the due date is a bit of mathematical nonsense, where people say things like “your baby is expected on 1 February, but will probably be late”. The due date is a slightly arbitrary number set at 40 weeks in the UK and USA and 41 weeks in France. No adjustment is made for it being your first, second, or later pregnancy, even though the distributions are quite different, so it’s not an “expectation” in any kind of statistical sense. Oster says the best way to know if baby is coming soon is to measure cervical dilation – which of course, in the UK, we don’t do.
I am not going to talk about labour (and the excellent care staff we met). It’s fascinating in its own way, but too personal, and this is a review of pregnancy, not childbirth. Fast forward a number of hours, and I was sitting uncomfortably by my wife again, this time with her sleeping in a regulation adjustable hospital bed and me perched on a bedside chair. And there, on a second bed, much smaller, with perspex walls and a 3-inch thick mattress, was baby. Hello, world.
Third Trimester Rating: 1/5. Weak direction and chaotic scripting, but final scenes unforgettable. Leads straight into sequel with insufficient break.
Overall Pregnancy Rating: 2/5. And yet, it’s one of the best things that’s ever happened to us.
– END –
Footnotes
- ↩
The NHS will give you an Early Pregnancy Scan if you present with symptoms (and are triaged towards the front of the queue relative to other patients on the day), but won’t give you a screening test before that point. See https://www.nhs.uk/conditions/ectopic-pregnancy/
- ↩
I say “implicitly” because on page 96 Oster calls Debendox the “first line of defense”, while noting it was taken off the market in the USA and never came back, despite studies not finding it to be dangerous. Something similar now seems to be available again, under the name Diclegis.
- ↩
In which case our hospital would hook the mother up to a machine for contraction and baby monitoring, potentially followed by an extra ultrasound and the ‘single deepest pocket’ test (Oster’s preferred test) for amniotic fluid levels.
- ↩
Oster (2013) Expecting Better
- ↩
Oster (2013) Expecting Better
-- END OF FOOTNOTES --