In 1999, Professor Clark Elliott is rear-ended by a stranger at a stoplight. He’s shaken but figures he’s fine, and drives to work. Spoiler: Clark Elliott is not fine.
Elliott is severely concussed, and this fact will dictate the next ten years of his life. Elliott’s memoir is based on notes he took while concussed. Reading it is like watching someone try to troubleshoot their broken laptop using the broken laptop.
In the opening chapter, Elliott describes walking from his office to his car after a long winter workday:
“At this point my world had collapsed inward on itself… I looked down at my feet and shouted at myself to walk, but I knew it was hopeless. I had lost the mysterious initiative that impels us all forward when we walk, and I knew that without brain rest I wouldn’t be getting it back. I considered lying down in the snow.”
Over an hour later, Elliott finally manages to cross the parking lot and begins the second phase of his trial: getting into the car.
“I’d lost the concept of center. I had no internal representation, or visual understanding of circle, target, middle, inside. Without these concepts I couldn’t get my hand to move toward the lock, or put the key in the slot.” So he just stands next to the door for another hour and a half.
Around 2 a.m., a suspicious police officer asks why Elliott is loitering in the parking lot, but the officer is too cold to get out of his car and drives away. At 3:30 a.m., four and a half hours after he left his office, Elliott finally arrives home.
Somehow, Elliott lives like this for a decade.
The book’s first mystery is how a person can remain conscious, verbal, employed, and yet so damaged that he can’t get into a car or recognize his own house. The second mystery is: why did he apparently recover through treatments that sound, at first pass, like boutique neuro-quackery?
A disclosure is in order before we continue. I am pretty personally invested in the answers here. About a year and a half ago, I got seriously concussed. Milder than Elliott's, but bad enough to substantially rearrange my life. On some level, I read this book in hope of a cheap fix, or at least an obvious one. Instead I found myself in the weird borderlands of modern medicine.
A hurricane let loose on 50 million desktop computers
What’s it like to be a human with severe brain damage? Elliott offers a metaphor:
To simulate concussion damage to a human brain then, we’ll need to gather together […] 50 million desktop computers, a 500,000-mile-high stack of paper, and the almost inconceivable amount of information it takes to construct a human mind, then loose a hurricane on the system, ripping out network lines, laying waste to vast sections of memory, and sending landslides to smash hundreds of thousands of computers.
A bit sensational, but you get the picture. One classic model of what’s happening during severe concussions is “diffuse axonal injury”: rapid acceleration and deceleration stretch axons, the neuron projections that send electrical signals, causing micro-tears and disrupting cellular metabolism.
Standard CT and MRI imaging usually fail to detect these microscopic or functional disruptions, and there isn’t really a cure, so patients are told to go home, rest up, and wait to find out whether they’ll be back to work the next day or out of commission for the next decade.
U.S. concussion incidence is commonly cited around 1.6-3.8 million a year, and many go unreported [1]. About 15-30% of adults report post-concussion symptoms (PCS) 3-6 months later. Even on conservative estimates, that’s hundreds of thousands of cases a year in the US alone. A much smaller number of those cases will result in something like Elliott’s experience.
After the initial fender-bender, Elliott hands his driver’s license to the other driver. Then, a few minutes later, he hands it over again. He has no memory of having done so the first time, and can’t figure out why people are looking at him funny. This is a recurring theme—Elliott can’t even notice the problem, because the cognition that’s supposed to monitor the behavior has gone offline.
He writes: “when cognitive capabilities go missing they are often so fully gone that the concussive does not miss them in the way a normal person would, or indeed sometimes even realize they’ve gone absent.”
But Clark Elliott is no pushover. He’s a Professor of Artificial Intelligence at DePaul University, a consummate musician, is single-handedly renovating his family home, and runs marathons on the side. The biographical lists serve a purpose: Elliott wants to assure the reader that he hasn’t become less intelligent. His cognitive capacities have just come apart in a way that doesn’t track any nameable cognitive disorder.
He can write, but he cannot read. He can climb stairs but not descend them. He can teach a graduate seminar and then, walking home afterward, fail to recognize his own house. Moving through doorways or down halls poses a significant challenge.
More than once, he describes his state as “alien.” He writes, “we still walk and talk and act as though we are part of the human race, but it doesn’t feel that way inside… Instead, there is a strange feeling of nostalgia, a longing for who we used to be.” He notes that this feeling of disconnection is likely a significant contributor to the rate of suicide among concussives [2]: “we have, in many ways, already lost that which makes us human.”
One of the most striking passages in the book is when Elliott, hungry, decides to make himself a snack. He heads to the kitchen to eat a piece of salami and an apple, but finds he can’t. As though trapped in an old Tom and Jerry cartoon, he finds himself literally unable to choose which of the two to eat first. He can’t initiate action selection. He goes to the living room, returns to the kitchen, fails again. He repeats this loop ten times, like “a rat repeatedly traversing a dead-end maze.” Two days pass before he eats.
Elliott calls this “getting stuck.” The bridge between knowing what he wants to do and doing it has broken. In desperation, he finally calls his bemused friend Jake, who tells him: “Okay, go eat the salami first, then eat the apple,” ending the forty-eight hours of struggle.
Somehow, he cobbles together enough coping mechanisms to keep limping along for years. Until he can’t anymore.
Partial death
“This is it,” Elliott reflected. “I am never going to have another normal day, or hour, or ten-minute period again. I am never going to be a real human being again. I won’t be publishing my research, and at some point I am going to lose my job.”
Ten years after the crash, Elliott is approaching a complete breakdown. Or rather, while broken, he adds a small child to the equation. As it turns out, the normal prattle of his two-year-old daughter is concussion kryptonite:
“It was this simple combination—my inability to filter out or process spoken dialogue in real time, and Erin’s continual need to talk—that almost led to a final, catastrophic meltdown.” He calls it “partial death.”
Unfortunately, there are no parenting sabbaticals. In a last-ditch effort, Elliott pulls out his emergency savings and reaches out to a “cognitive restructuring specialist” named Donalee Markus.
Wait a minute, you might be thinking. Elliott hasn’t seen a specialist before??
He has, sort of. It didn’t help. A brief detour through medical history: Elliott hit his head in 1999. The CDC didn’t publish its first major report on mild traumatic brain injury (TBI) until 2003. The NFL concussion crisis broke into public awareness in 2005. Until 2013, the only mention of persistent post-concussive symptoms in the DSM-IV was in the appendix under “proposed criteria set”. After the crash, an ER doctor checks his pupils and sends him home; a neurologist runs a 30-minute test and declares him fine, and shouts at him when he pushes back.
It’s unclear whether Elliott was just unlucky in encountering a cast of extremely unsympathetic medical professionals, or whether this was really the general state of neurology in the 90s. Whatever the case, Elliott quickly writes the whole system off and goes back to calling his friend Jake whenever he gets stuck in doorways.
The Miracle Begins
For ten years, Elliott can’t make himself a sandwich. Then, over the course of a year, he substantially recovers. Enter idiosyncratic concussion specialists Donalee Markus and Deborah Zelinsky.
This is the first time we have a third-person perspective on Elliott. Markus writes:
“Clark Elliott was a mystery to me when we first met. Observing him through my glass front door, I saw that it took him two minutes just to find the doorknob with his hand. When I gave him the simplest of my assessment tests—copying a geometric line drawing—his body went into bizarre contortions as he struggled to complete it.” Markus takes him on as a patient anyway.
Her intervention is simple: she gives him geometric puzzles to solve, specifically trapezoids and three-dimensional dot exercises that escalate in complexity. He has to apply rules to shapes, generate equations from them, and eventually do the whole thing in his head.
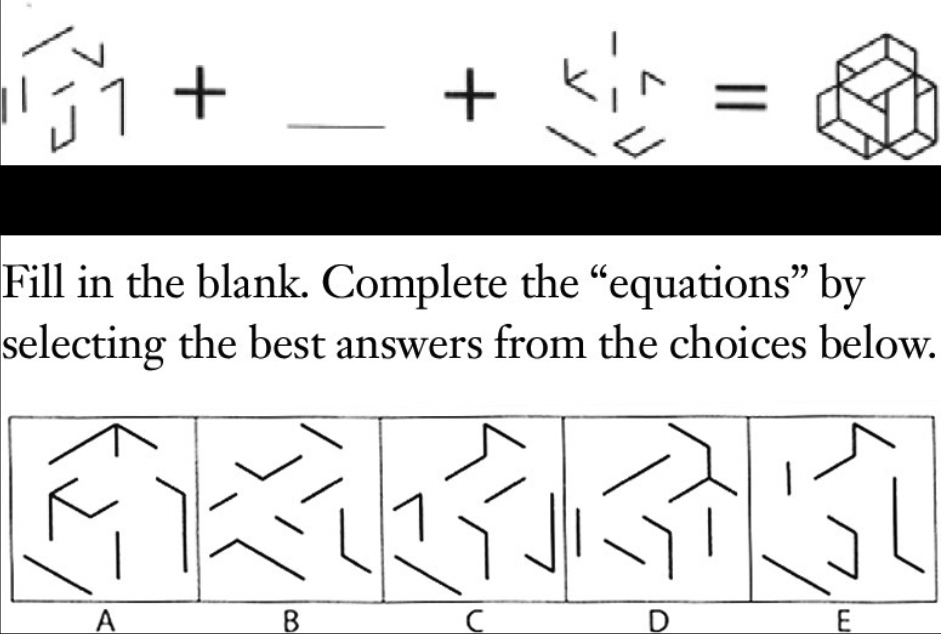
(Source): Elliot includes a bunch of these geometric puzzle examples in the book. Sadly, they didn’t alleviate my symptoms.
Markus also refers Elliott to her colleague Deborah Zelinsky, a neuro-optometrist.
Bells and Prisms
Zelinsky's diagnostic method is a little more involved. The patient closes their eyes, and the examiner rings a small bell at various positions in space. The patient must reach out to touch the bell. The patient will often fail this test, revealing a “visual-auditory mismatch.” Zelinsky will then try different prism lens combinations while the patient's eyes are closed and ask them to do the bell test again. I repeat, the patient’s eyes remain fully closed. The entire time. She then prescribes the lenses that improve the patient’s performance. 
(Source). The only image I could find of the Z-bell test; fittingly grainy and hard to evaluate.
This is called the Z-bell test (presumably after “Zelinsky,” who has a patent on it). While I wasn’t particularly surprised that adjusting someone’s vision when their eyes are open can change how accurately they localize sound when their eyes are closed, I remain deeply confused about how prism lenses could alter accuracy if the patient’s eyes remain closed the entire time.
The claim is that low-level light still passes through the closed eyelids, stimulates retinal activity, and that this stimulation is what’s being modulated by the different lenses.
Zelinsky’s Mind-Eye Institute website:
“By placing various types of lenses across a patient’s closed eyes, we can change the way light spreads over the retina, thus modifying the dynamic relationship between the mind’s visual inputs and the body’s internal responses.”
Depending on wavelength, eyelids transmit somewhere from well under 1% of blue/green light to around 5–6% of red light. But, as anyone with eyelids knows, this is still mostly diffuse reddish illumination—not sufficient to update your visual field, or to localize a bell.
But within a year of meeting Markus and Zelinsky, Elliott has experienced massive improvements and is on the road to recovery. He writes a heartfelt note to Markus thanking her for “giving him his life back.” So I guess the treatments worked?
Into the uncanny valley of concussion science
Let’s take a look at the evidence, starting with Markus. Markus belongs to a fairly large tradition of “cognitive training interventions” for PCS for which there’s some evidence. A 2016 meta-analysis looking at 14 studies on cognitive training in post-acute TBI found a small effect on overall improvement in cognitive function (Hallock et al., 2016).
Unfortunately, “cognitive rehabilitation" is an enormous umbrella and Markus's specific protocol isn't in the meta-analysis. Markus published her own protocol in 2007, describing the puzzle-based technique she used on Elliott, but it’s more of a “how I do it” piece, not a controlled trial. The trail of scientific evidence dries up there.
Okay, what about Zelinsky? Do the bells work? There’s a 2019 paper that tried to find out. First author: Clark Elliott.
The paper is a preliminary conference paper on 14 out of the 41 recruited participants. Elliott et al. find that the therapeutic lenses produced a small but statistically significant improvement in bell-touching accuracy compared to the clear-lens baseline. However, the therapeutic lenses didn’t outperform an ‘impaired lens’ condition, which was theorized to push the outcome in the opposite direction, and the full study with all 41 recruited participants has never been published.
This is pretty tepid evidence. With one preliminary, ambiguous analysis its only empirical bulwark against the wave of scientific skepticism, Zelinsky's method isn’t looking too good.
That said, the testimonial evidence is abundant. “I can move normally again, be active, travel. Mind-Eye has opened up a whole new chapter in my life,” says an avid patient. One testimonial describes the treatment as “like, well, ‘magic,’” while another patient calls it “mathemagical.”
We can add Clark Elliott to the rave reviewers. Within ten days of his first prism glasses, he reports a strange shift. Music sounds different, and he starts re-accessing visual scenes from childhood.
Within a month, Elliott begins to feel like himself again. The “ghost of his true self” had reentered the room. “At last I had enough brain power to support the real me, the complex me. I could see the world through my own eyes again.”
The strongest within-book evidence that the glasses, in particular, are doing causal work comes from what happens when Elliott briefly loses them. Even 33 hours without his prescription produces dramatic regression: exhaustion, handwriting deterioration, visual disturbances, and the return of the “all tasks involve pain in some way” baseline of his pre-recovery life. Once he finds the glasses, he’s back to playing the Beatles from memory and “looking forward to the rest of [his life] again.”
Elliott is writing the book fifteen years after the accident, and the recovery has held. He even claims, with the partial qualification one expects from a man who has nearly lost his mind to a brain injury, that his cognition is in some ways now better than it was before the crash.
A skeptical explanation might be that Elliott was desperate and ripe for placebo effect. Receiving intense attention from clinicians who believed they could help him after years of failed encounters with doctors might have been sufficient to shift his symptoms. Elliott's recovery was staged over five years with iterative adjustments, which is exactly the protocol that would maintain a placebo effect, and the base rate of spontaneous recovery in chronic PCS is non-zero. So can we be sure that any of these treatments did anything other than give him a pat on the back as the concussion worked itself out?
I think a case can be made for at least some real intervention. While the evidence for Zelinsky’s closed-eye method in particular is thin, the general “prescribe new lenses” approach looks much more promising. There’s even a reasonable causal mechanism on offer.
If you hold up your thumb in front of your face, and then easily switch between looking at something on the wall and your thumb, congrats - your accommodation triad is working. The accommodation triad is the trio of ocular functions that enable close-up vision. In many PCS patients, this system goes awry, resulting in a suite of vision complications. In a study of adolescent patients (n=116), Wiecek et al (2021) found that ~60% of patients had deficits in near point of convergence after concussion. Prism lenses can reduce eye strain by shifting the image on the retina so the eyes don’t have to work as hard to converge, and magnifying lenses reduce accommodation demand.
A year into my concussion, and partially inspired by Elliott, I asked my neuro-opthalmologist for prism lenses. They didn’t help at all. But the magnifying lenses I tried next totally did, almost entirely eliminating my symptoms immediately (unfortunately, they later returned).
It’s possible that Zelinsky’s method actually does work, but not for the reason she thinks. The bell ceremony might just be an unusually elaborate way to arrive at a genuinely useful prescription.
This would explain both her rave reviews and the lack of scientific support. Her Z-bell tinkering isn’t doing much, but the broader lens intervention sometimes works—some percent of the time, prism glasses and magnifying lenses actually do improve people’s concussion symptoms. (Of course, this will result in a hit-or-miss treatment, but you can’t tell because none of the duds post a review).
When averages fail
So what, if anything, can we learn from Elliott’s recovery?
Here’s one obvious point: recovery is possible, but strangely elusive. It took Elliott a decade, several awful medical encounters, and two boutique specialists to find help. While the situation was worse in the 90s, it’s still bad today. In one study, among patients severe enough to reach specialty care, fewer than a third had recovered when surveyed, and the still-symptomatic group had been living with PCS for an average of 4.5 years (Hiploylee et al., 2017).
Perhaps the real mystery is: why is it so hard to treat concussions?
One reason is that concussions resist mainstream medical intervention. Clinical instruments can’t catch the microscopic damage common to PCS, and randomized controlled trials (RCTs) struggle to identify treatments when the population is heterogeneous and the symptoms are varied and subjective. So it takes months to get a PCS diagnosis, and even when you do, many clinicians have no idea what to do with you.
PCS treatment is hard because concussion does not damage an abstract, average brain. It damages your brain, with your particular foibles and weak spots. Specialist concussion medicine has identified roughly six clinical phenotypes, but even when correctly type-cast, each patient responds differently. Clark Elliott and I both had vision issues, but he responded to prisms while magnifying lenses worked for me. PCS may be less like a single disease than a family resemblance category with wildly different failures compressed into one diagnosis.
RCTs are the “medical gold standard.” But perhaps idiosyncratic medical maladies are where the standard hierarchy of evidence breaks down a little. Philosopher of science Nancy Cartwright has argued that RCTs answer a narrower question than clinical practice needs: they tell you that a treatment, on average, produced a particular outcome in a trial population. They don’t tell you whether it will work for you in particular.
So PCS patients navigate the uncanny valley of niche medical science: on the one side, RCTs and rigorous studies that document average effects that might not apply to you, and on the other, N=1 case studies that might solve your exact problem, or be entirely useless. In the middle, there’s a bunch of people trying to sell you metabolism-enhancing lasers for five thousand dollars. Absent clear explanations, patients can find themselves passed between neurologists, optometrists, physical therapists, vision therapists, acupuncturists, psychiatrists, and energy-healers before finding the one thing that happens to work for them.
To get the most juice out of a clinical trial, you need a theory of why the treatment worked, for whom, and whether you’re similar enough to the trial population for the effect to transfer.
But what if you don’t have a mature theory yet?
Z-bell tests and Fijian reef fish
As a species, we’ve been solving problems we don’t understand for a long time. On Fiji’s Yasawa Island, pregnant and breastfeeding women observe taboos against eating certain species of reef fish. When Natalie and Joseph Henrich investigated in 2010, they found that the taboo species mapped onto the fish most likely to carry ciguatera toxin, a naturally occurring marine toxin that’s particularly dangerous to fetuses and nursing infants. Local variation combined with fitness-relevant outcomes and social learning can surface solutions long before the mechanism is understood. (The trade-off is that sometimes they suggest you try bloodletting or child sacrifice).
For poorly understood chronic conditions, treatment often looks less like applying established science and more like janky cultural learning. PCS communities generate variation, share outcomes online, and copy apparently successful interventions.
But what makes the Fijian case work is that there’s a real selector pulling signal out of the noise. Toxic fish made people visibly sick, and useful taboos could be reinforced across generations. The PCS testimonial ecosystem has no comparably reliable selector; variants can propagate just because they’re dramatic or recent or someone’s trying to sell you something. The same dynamics that make it kind of reasonable to try Zelinsky’s Z-bell test might push you toward forty sessions of hyperbaric oxygen at $200 a pop.
Another drawback is that cultural transmission is good at producing outcomes, but overimitates methods. The Z-bell case is actually a nice illustration. Even if Zelinsky's lenses actually help some patients, the community's causal story (closed-eye retinal stimulation) might be totally wrong. Cultural transmission will faithfully convey the bells-and-mathemagic ritual along with whatever genuinely works.
Alright, clearly we can’t just trust the forums. In an ideal world, we’d capitalize on the strengths of patient communities (lots of people trying lots of things) and combine it with some kind of rigorous selection mechanism.
Luckily, there's already a proof of concept for this. In 2020, the Body Politic COVID support group pioneered a novel idea: ask patients stuff. They created the Patient-Generated Hypotheses Journal (PGHJ) and began advising (and funding) major research efforts. Their flagship peer-reviewed paper (Davis et al, 2021), an online survey of 3,762 people drawn from support groups across 56 countries, found that Long COVID affected multiple organ systems, that symptoms persisted well past acute infection, and that recovery often took many months (all borne out by subsequent research).
Some community-amplified hypotheses won’t hold up—great, that’s what science is for! At the least, the PGHJ demonstrates that heterogenous patient communities can do more than swap miracle stories; they can generate structured observations and funnel hypotheses toward controlled studies. For example, do prism glasses actually improve general cognitive functioning in PCS patients with convergence issues? Despite Elliott’s popularization, as far as I can tell there are literally no RCTs testing this.
For medical orphans like PCS, the evidence hierarchy is doing the right things in the wrong order. Population-wide RCTs belong at the top once we know what outcome we care about and what mechanism we’re targeting. Until then, structured patient case registries could help us figure out what actually deserves a trial.
Getting out of the parking lot
Two years ago, if someone asked me how to navigate PCS, I would have said, “Uh, only pursue treatments with clear, scientifically-backed benefits.”
And at first, that’s what I did. My path to recovery started with best-evidenced treatments. But as the months dragged on without improvement, I found myself in testimonial-land—trying things based on Google Maps reviews, and reading this book.
As a concussion roadmap, The Ghost in My Brain is pretty frustrating. Elliott is too ready to accept his clinicians’ explanations and treats his recovery path as way more generalizable than it is. But as phenomenology, it’s excellent. It does a great job of conveying what it feels like when your brain breaks. If you’re intrigued by the extreme edges of human experience, this is for you. If you’re looking for a guidebook, sorry, there isn’t one (yet).
For conditions like severe, persistent PCS, the patients who recover often fall into two groups: the ones who are lucky enough to find clinicians willing to iterate with them, and the ones who have the time and money to experiment on themselves. That’s a small slice of the population.
We can’t just replace RCTs with facebook groups, but maybe we could bridge the weirdness of individual cases and the discipline of controlled science. The rather dark irony here is that the PCS patient community has PCS. Many of us can’t look at screens, nevermind organize case registries. But if even the conservative end of the PCS estimates is right, that’s hundreds of thousands of cases a year. Many of those people are doing exactly what I did—trawling through forums and trying treatments. And whether or not anyone records the results, people will continue to search the solution space. Because when your brain breaks and you’re stuck in apple vs salami hell, you try all the bells and prisms.
Your message is stored now and emailed to the author after the contest ends. The author can reply to you, but their identity stays hidden unless they choose to respond.
Footnotes
- ↩
Institute of Medicine and National Research Council. Sports-Related Concussions in Youth: Improving the Science, Changing the Culture. National Academies Press, 2014, citing Langlois et al. 2006. This is technically a report on sports and recreation-related TBI and concussion, which are overlapping categories that both often lead to PCS. Given that this is just sports and rec related, the real number must be much higher.
- ↩
A major JAMA Neurology meta-analysis found a relative risk of suicide of 2.03 after concussion/mild TBI. In two included cohort studies with about 4 years median follow-up, suicide deaths occurred in 0.50% and 0.59% of diagnosed concussion/mTBI patients. That is roughly 1 in 200 over that follow-up period